
Research ArticleOpen Access, Volume 3 Issue 1
Marburg virus disease in sub-saharan Africa: Contemporary epidemiology and future trends
Olusola Bamidele Ojo*
Medical Registrar, Health Care Agency, Ministry of Health, Seychelles.
*Corresponding author: Olusola Bamidele Ojo
Medical Registrar, Health Care Agency, Ministry of Health, Seychelles.
Email: ojoolusola302@gmail.com
Received : Feb 24, 2025 Accepted : Mar 19, 2025 Published : Mar 24, 2025
Epidemiology & Public Health - www.jpublichealth.org
Copyright: OJo O © All rights are reserved
Citation: Bamidelej OJo O. Marburg virus disease in sub-saharan Africa: Contemporary epidemiology and future trends. Epidemiol Public Health. 2025; 3(1): 1065.
Abstract
There is a recurrent rate of filoviral epidemics including Marburg virus disease and its concomitant high mortalities in recent times. Thus, the need for prompt control of their outbreaks has never been greater, especially in sub-Saharan Africa. Given the severe economic and social catastrophe of the COVID-19 pandemic, the world needs to mitigate a recurrence by stemming outbreaks of high-risk pathogens with pandemic propensities like the Marburg virus. Therefore, we deployed a rapid systematic review of relevant secondary sources on Marburg Virus Disease, tracing its historical epidemiology and exposing its current situation in sub-Saharan Africa. We found an average case fatality ratio of 23 to 100% between 2004 and 2025. Hence, we argue that the mortalities ascribed to Marburg Virus Disease are comparable to Ebola. Thus, this piece reemphasizes the need to focus on community education and engagement and intensify the world’s focus on discovering vaccines against Marburg Virus Disease like Ebola and COVID-19.
Keywords: Marburg virus; MVD; Sub-Saharan Africa; Ebola; EVD; Epidemiology.
Introduction
As humans continue to encroach into the sacred sanctuaries of wild animals in the post-modern world, the frequency of contacting high-risk pathogens from animal vectors continues to soar. In the post-COVID-19 pandemic era, many high-risk infectious agents continue to occasion morbidities and mortalities of public health significance. Filoviruses such as the Marburg virus and Ebola virus cause highly contagious infections characterized by a high fatality ratio. They belong to a group of hemorrhagic fever viruses, specifically characterized by hemorrhagic clinical complications with antecedent high fatalities. Other causes of viral hemorrhagic fever include dengue, zika, chikungunya, Lassa, and Congo-Crimean. In sub-Saharan Africa, Marburg Virus Disease (MVD) killed 59 people between 2021 and 2024 in Ghana, Guinea, Equatorial Guinea, Tanzania and Rwanda [1]. As of 15 January 2025, with patients manifesting the clinical symptoms of the contagion from 10 January, Marburg has claimed another eight lives in northwest Tanzania [2]. The frequency of MVD in sub-Saharan Africa has surpassed other regions of the world probably due to the abundance of its vectors and unavoidable contacts of humans with its carriers [1]. Marburg virus and Ravn viruses are the usual cause of MVD. In 2022, MVD among other hemorrhagic viral diseases were identified as one of the high-risk factors that could trigger another devastating pandemic in the future [3].
Marburg and Ebola viruses are highly virulent and contagious pathogens that belong to the filoviral family [4]. Marburg virus was extracted and sequenced in the German and Serbian laboratories, thought to have emanated from monkeys imported from Uganda in 1967. The virus was later named after the city where the virus first affected people in Marburg, Germany [5]. Since then, this extremely virulent pathogen has been responsible for different fatal outbreaks till the turn of the 21st century [6]. However, only a handful of cases were recorded in sub-Saharan Africa between 1975 and 1985. However, since the fatal epidemic occasioned by Marburg virus in 2000 in Congo DRC, the contagion has posed a continuous significant threat to public health in contemporary Africa. For instance, according to World Health Organization data, from 2004 to 20 January 2025, sub-Saharan Africa has witnessed 10 outbreaks. There were 516 MVD cases with 398 deaths [1]. Comparatively between 1975 and 2000, there were only four outbreaks due to the Marburg virus with a total number of 160 people affected, out of which 131 died [1,7].
These epidemiological values underscore the substantially high fatality rates of MVD as well as its frequency of outbreaks in contemporary sub-Saharan contexts. The average case fatality ratio of MVD is 50% with variations between 24 and 88% putting past epidemics into perspective [1]. The menace of MVD compares with Ebola Virus Disease (EVD) in fatalities as recent epidemics had up to 90% death rates compared to Ebola Outbreaks of 2014/15 in West African contexts. For instance, a case fatality ratio of 83% was recorded in Congo DRC, and Angola recorded a fatality rate of 90% in the recent era [4]. Similarly, in 2022, in the Guinea outbreak, nine out of ten infected patients died from the contagion [8]. More recently, and in the post-COVID-19 pandemic period, sub-Saharan Africa had witnessed a series of outbreaks with devastating morbidities and mortalities. From 2022 to 2024, MVD killed 56 people out of 115 victims in Rwanda, Tanzania, and Equatorial Guinea [1]. There are obvious human and environmental factors, which enhance recurrent Marburg virus outbreaks in present-day Africa. There is an abundance of green monkeys and Egyptian fruit bats (Rousettus aegyptiacus), which harbor the Marburg virus [9]. The economic realities of some sub-Saharan necessitates interaction with bats in mines and caves [5]. Wars and instabilities remain another trigger of high pathogen outbreaks in sub-Saharan Africa. As of January 2025, following the fall of Goma resulting from coordinated offensives on Congo DRC by M23 faction, there is a heightened risk of regional conflicts and widespread socio-economic dislocations [10,11]. Consequently, there could be recrudescence of EVD and MVD with accompanying substantial mortalities in the region.
There is no paucity of research regarding filoviral diseases including MVD in the regional and global settings. Several researchers have highlighted its global threats of the virus due to the precariously high case fatality rate of the virus [12-14]. They specifically highlighted the regional threats of Marburg virus, which could transmigrate to global pandemic given the fluid transportation and the economic necessities of the tourism and mining sectors in some sub-Saharan climes. These expose people to the reservoirs of the virus, hence risking contracting the deadly disease and dispersing it to local populations. The flourishing tourism and mining sectors are economic blessings but banes regarding the swift transfer of high-risk pathogens such as the Marburg virus to distant regions. Concerning the recognized carriers of the Marburg virus, some scholars have identified green monkeys and fruits bats as the main transporters of the Marburg virus because of evidence of past outbreaks supported close contacts with them. Some scholars have ascribed fruit bats, Rousettus aegyptiacus, as the main reservoir of the Marburg virus [13,15]. They suggested that horizontal transmission, which involves the dispersal of the Marburg virus among bats as well as vertical spread from contacts with bats to human are plausible. Bats could transmit virus to themselves through bites and sexual relations [16,17]. Subsequently, infected humans transmit the virus directly via infected body fluids like blood, saliva, feces, vomitus, breastmilk, amniotic fluid, and seminal fluid. Indirect transmission has been documented via contaminated surfaces and materials, such as clothing, bedding, and medical equipment. Like Ebola virus, infected bush meats such as chimpanzees and forest antelopes, whether dead or alive could transmit the Marburg virus [18,19]. However, the bush meats cannot serve as reservoirs like bats, because once afflicted with the virus, they usually die. Hence, they serve as intermediate hosts to the Marburg virus, and infected dead human bodies could transmit the Marburg virus [18-20].
Some studies focus on the viral properties and the clinical manifestation of the Marburg virus [21-24]. Marburg virus is a negative R.N.A sense virus, which displays a filamentous, rod- like, non-segmented, and branched particle patterns on characterization [25,26]. It belongs to the genus Marburgvirus of the family Filoviridae [27]. Regarding the clinical manifestation of Marburg virus victims, the incubation period is usually two to 21 days, and there are three different phases of affectation. The first stage, generalization phase, starting from day two to five after the outbreak of symptoms. It is characterized by fever (>40°C), chills, myalgia, strong headache, and weakness. There were documented manifestations of malaise, anorexia, nausea, vomiting and abdominal pain [28]. Other plausible clinical features of the first phase include pharyngitis, conjunctivitis, enanthem, and maculopapular rash. The rash, usually non-itchy, commonly develops within two to seven days of the commencement of symptoms [29]. The second phase lasts from day five to 13 from the inception of symptoms. It is characterized by a prolonged phase of fever and hemorrhagic manifestations. Roughly 75% of sufferers develop hematemesis, ecchymosis, melaena, petechiae, bloody diarrhea, vaginal bleeding, epistaxis, and uncontrolled bleeding from venipuncture sites [13]. The third phase, which is the late stage, could either result in death or prolonged recovery. Mortalities due to the Marburg virus usually happen from day eight to day 16 after the commencement of clinical manifestation of the disease. The main causes of death are severe dehydration, anuria, metabolic disturbance, and multiorgan failure [5,13].
Regarding the theme of this piece, only a few scholars have focused on the current epidemiological trends of MVD in sub-Saharan Africa. Some researchers have traced the historical trajectory and epidemiology of Marburg, albeit from global perspectives [7,12,13,30]. However, only few researchers have focused on the peculiarities of the contemporary sub-Saharan Africa regarding the unfettered and uncontrolled disease outbreaks in the contexts of Marburg virus [31,32]. One recent study highlighted the prevalence of MVD and EVD in sub-Saharan but did not elaborately focus on Marburg’s other epidemiological attributes in present-day settings [33]. There is varied epidemiological data on MVD in contemporary sub-Saharan Africa. Hence, there is a need for a study to harmonize the existing prevalence data on MVD. This would display the widespread threats of the pathogen in the whole sub-Saharan geographical context. This would heighten our understanding regarding the threats of MVD to regional and global health. It would help us to offer research-backed recommendations to mitigate recurrent scourges of highly contagious diseases including MVD in contemporary sub-Saharan Africa. Hence, the emphasis of this study is on delineating current epidemiological trends in sub-Saharan Africa.
Methodology
We deployed a rapid systematic review for this study. We searched three databases, namely Google Scholar, PubMed, and Web of Science about articles regarding MVD since its emergence in 1967. We set up a research question regarding the emergence, precipitating factors, epidemiology, and management of MVD. To refine our examination, we used keywords such as Marburg, Marburg Virus, Marburg Virus Disease, and Marburg virus epidemics. Only peer- reviewed journals relevant to our research area were deployed and analyzed for this study. Eligible studies must be original primary research from peer-reviewed papers reporting the patterns, distribution, prevalence, precipitating, or enhancing factors of MVD and its outbreak in humans. We did not deploy studies conducted outside of sub-Saharan Africa. Moreover, we selected relevant articles and suitable references from them via snowballing.
Epidemiology of marburg virus in sub-saharan Africa, 1967-2000
This study focuses on the epidemiological characteristics of MVD in sub-Saharan Africa. In this light, we will display a comprehensive table of epidemiology of MVD in the past era, from 1967-2000. This would enhance adequate comparison with the epidemiological attributes of MVD in the 21st century. (Table 1) shows the epidemiological features of MVD between 1967 and 2000.
Table 1 displays the epidemiological attributes of MVD from 1967 to 2000. It shows the approximately equal prevalence of MVD in the central, eastern, and the southern parts of Africa. However, Congo DRC had the highest number of MDV cases and mortalities due to the dire humanitarian impacts of the Second Congo War between 1998 and 2003 [34]. The average case fatality ratio from 1967 to 2000 was 83.6%. All the affected countries had a zoonotic transmission of Marburg virus before human-human contacts predominated as the main transmission route.
Table 2 shows epidemiological attributes of MVD in contemporary sub-Saharan Africa. Compared to (Table 1), from 2004 to 2024, Africa witnessed MVD cases in the usual southern and eastern belts of MVD. However, there were recorded cases in the new blocs. Equatorial Guinea at the fringes witnessed MVD outbreaks with devastating fatalities in 2023. In 2021, Guinea encountered an MVD outbreak, the first in the annals of a West African country. Ghana became the second West African country to declare an MVD outbreak in 2022, losing two lives to the contagion. It indicates that MVD might be pervading unknown areas of significance in sub-Saharan Africa. Table 2 shows that the case fatality ratio of MVD ranges from 23 to 100%. It is consistent with available data on the approximate case fatality ratio for MVD. However, the average case fatality ratio of 76.6% from 2004 to 2025 is marginally lower than 83.6% computed between 1967 and 2000. Exposure to Rousettus Aegyptiacus remained the dominant route of contracting Marburg virus. Nevertheless, exposure to wild games remained plausible in the Guinea and Angola contexts due to the existence of large forests replete with wild games.
Table 1: Epidemiological characteristics of Marburg virus disease between 1967 and 2000.
| MVD epidemics | Location | Source of Marburgvirus | Number of cases | Number of deaths | Case fatality ratio(%) | References |
|---|---|---|---|---|---|---|
| 1975 | South -Africa | Rousettus Aegyptiacus | 3 | 3 | 100 | [35,36] |
| 1980 | Kenya | Rousettus Aegyptiacus | 1 | 1 | 100 | [36] |
| 1987 | Kenya | Rousettus Aegyptiacus | 1 | 1 | 100 | [36] |
| 1998-2000 | Congo DRC | Rousettus Aegyptiacus | 154 | 128 | 83 | [35] |
| Total | 159 | 133 | 83.6 |
Table 2: Epidemiological characteristics of MVD outbreaks, 2004-2025.
| MVDEpidemics | Location | Source of MarburgVirus | Number of cases | Number of deaths | Case fatality ratio(%) | References |
|---|---|---|---|---|---|---|
| 2004-2005 | Angola | Unknown | 252 | 227 | 90 | [36] |
| 2007 | Uganda | Rousettus Aegyptiacus | 4 | 2 | 50 | [1] |
| 2012 | Uganda | Rousettus Aegyptiacus | 23 | 15 | 60 | [38] |
| 2014 | Uganda | Rousettus Aegyptiacus | 1 | 1 | 100 | [1] |
| 2017 | Uganda | Rousettus Aegyptiacus | 4 | 3 | 75 | [22,36] |
| 2021 | Guinea | Unknown | 1 | 1 | 100 | [22] |
| 2022 | Ghana | Unknown | 3 | 2 | 66.7 | Huzain (2022) |
| 2023 | Equatorial Guinea | Unknown | 40 | 35 | 87.5 | [7] |
| 2023 | Tanzania | Unknown | 9 | 6 | 66.6 | [1] |
| 2024 | Rwanda | Rousettus Aegyptiacus | 66 | 15 | 23 | [1,2] |
| 2025 | Tanzania | Under investigation | 9 | 8 | 89 | [2] |
| Total | 407 | 312 | 76.6 |
https://www.gettyimages.com/detail/illustration/marburg-virus-cut-away-illustration-royalty-free-illustration/1205739663?adppopup=true

https://www.gettyimages.com/detail/photo/egyptian-rousette-royalty-free-image/1220806653?adppopup=true
https://www.frontiersin.org/files/Articles/1239079/fmicb-14-1239079-HTML/image_m/fmicb-14-1239079-g005.jpg
Discussion
Rousettus Aegyptiacus has been acknowledged as the main source of index MVD cases from 1967-2004. Fruit bats reside mainly in the sub-Saharan clime, the predominantly hot and humid climate replete with dense forest provides abundant fruits for feeding and hence, breeding [35-37]. They are major transmission reservoirs to many viruses including the Marburg virus [38]. The suitability of Rousettus Aegyptiacus as hosts for various viruses are probably due to their genetic diversity, extensive terrestrial distribution, and social, biological, and immunological attributes [39,40]. However, the emerging incidences of unknown sources of infections in some recent outbreaks lend credence to the plausibility of other sources of MVD infections. Wild games such as monkeys, chimpanzees, antelopes, and bush rats might be responsible in such cases. Some evidence shows these mammals eat fruits initially consumed by fruit bats, consequently transmitting filoviruses to them [41]. The emerging cases in previously unknown Marburg geographical belt might be related to increasing urbanization and forest encroachments. This results in heightened exposure of humans to fruit bats and wild games in some sub-Saharan states.
Another notable enhancer of frequent high-risk pathogens outbreaks including MVD is socio-political unrest and hostilities, which usually occasion catastrophic humanitarian crises. The second Congo warfare from 1998 to 2003 [34], correlated with the period of human fatalities provoked due to MVD outbreaks in the country. Massive socio-economic dislocations, weakened health systems, and inevitable human exposure to reservoirs of the Marburg virus, are the major enhancing factors to infections and its concomitant mortalities.
The MVD fatality rate in the present era, 2004-2025, ranged from 23 to 100%. It is consistent with the WHO’s fatality rate of 24-90% because the study deployed past data on MVD outbreaks derived from WHO and other related sources [1]. Hence, the correlation. However, the case fatality ratio of MVD between 2004 and 2025, 76.6%, is slightly lower than the value from 1967 to 2000. It might be due to marginal improvement in disease preparedness, clinical suspicion, laboratory testing, and community awareness and engagement. For instance, in the Marburg outbreak in Guinea, in 2021, only one mortality was reported. The index case was promptly identified, contacts were traced, and the victims had hygienic burial to mitigate escalation to wider epidemics. The recent Rwandan outbreak in 2024, was relatively well managed with heightened contact tracing, community education regarding safe burial practices, and deployment of PPE for healthcare workers. Therefore, a 26% case fatality ratio was reported compared to higher values in previous MVD outbreaks [1].
Conclusion
MVD is an extremely virulent and contagious disease, capable of transcending regional boundaries to escalate to a devastating pandemic like COVID-19. Like the Ebola virus, the Marburg virus is a category A pathogen with Risk Group 4 pathogen [37], thus tends to trigger more devastating fatalities. Its frequent outbreaks in the contemporary era necessitated a scholastic review. Hence, we delineated past and present epidemics of MVD outbreaks regarding their epidemiological attributes. We discovered that the case fatality ratio of 83.6% between 1967 and 2000 was relatively higher than the 76.6% computed for outbreaks between 2004 and 2025. This might be due to a marginal community awareness and engagement of MVD leading to a slightly improved early case detection and disease preparedness in the contemporary era. However, we derived a case fatality ratio of 23 to 100% for MVD between 2004 and 2025. Likewise, EVD has a case fatality ratio of 25 to 90% depending on geographical contexts [42]. Therefore, we maintain that MVD has a comparatively high fatality ratio like EVD, and deserves similar disease preparedness, response, and vaccine research like EVD. Thus, all hands must be on deck to stem recurrent MVD outbreaks in sub-Saharan Africa.
Recommendations
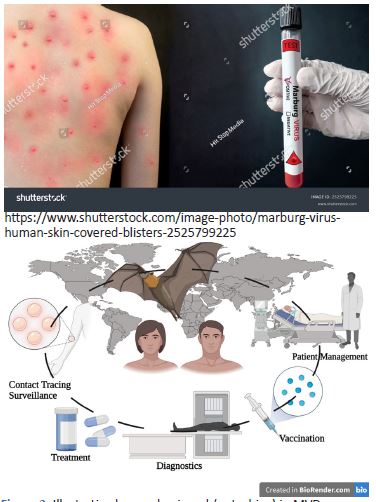
To mitigate frequent MVD outbreaks, there should be heightened community education about common sources of infection of MVD and the need for safe burials of Marburg dead bodies to mitigate escalations of infections. Local populations and tourists should be abreast of transmission reservoirs such as fruit bats and wild animals, and efforts should be made to minimize contact with them and their discharges. Miners and tourists should be equipped with hand gloves, face masks, and protective clothing when they visit mines and caves. Even though Egyptian fruit bats have been identified as the main reservoirs of the Marburg virus, we do not completely understand how they transmit it to other animals and humans. To comprehend these dynamics, we must intensify our studies on fruit bats. Bat surveillance should be strengthened to understand the migration, breeding, and transmission mechanism of Rousettus Aegyptiacus among themselves as well as wild animals and humans. This would further illuminate our understanding regarding the epidemiology of MVD to curtail its transmission to humans and hence prevent its epidemics.
There is no definitive treatment for MVD except rehydration and other conservative management. However, some antivirals such as Remdesivir and T-705 (favipiravir), which impair viral replication and transcription have a measure of efficacy towards MVD in non-human primates [43]. It is noteworthy to point out that their effectiveness and safety in humans remain untested. A major conservative regimen involves fluid rehydration and electrolyte replacement. Others relate to broad-spectrum antibiotics and fresh frozen plasma for secondary bacterial infections and bleeding dysfunction. They have proven beneficial to address some of the debilitating symptoms of MVD. Antipyretics have been pivotal in controlling continuous high fever. Sufferers must have adequate bed rest, be nursed in isolation, and be under strict supervision. As MVD is extremely contagious, healthcare workers must don the appropriate Personal Protective Equipment (PEP), gloves, and eye Google to prevent nosocomial infections.
Some vaccines are undergoing clinical trials, among which the Marburg virus vaccine known as mRNA-1,360 has shown promising signs against the virus. It is a dead virus-based immunization engineered from inactivated Marburg virus and specifically meant to enhance protection against MVD [44]. In the foreseeable future, apart from mRNA-1,360, we foresee the deployment of a definitive and effective vaccine as the main preventive strategy for tourists, miners, and local populations to redress the severity and transmission rates of MVD. Most sub-Saharan states have weak healthcare systems bedeviled by poor funding, inadequate healthcare manpower, and inadequate testing capacities for high-risk pathogens. To adequately manage the contagion, a quick and correct laboratory diagnosis is imperative. PCR, immunoglobulin M Capture ELISA, and Enzyme-Linked Immunosorbent Assay (ELISA) are critical to confirm the diagnosis of MVD [13]. Many sub-Saharan climes, most especially the rural and remote areas lack these laboratory capacities in their healthcare system. MVD’s early clinical features resemble other common tropical ailments such as malaria, typhoid, gastroenteritis, and others. This often delays adequate case identification and subsequent diagnosis, hence enhancing the transmission of MVD. This consequently heightens mortalities due to MVD. In this light, there is an urgent call for the healthcare system to strengthen with adequate funding and capacity building to stem MVD recurrent outbreaks in sub-Sahara Africa. It behooves many sub-Saharan economies to enhance the capacities of their infectious disease surveillance and laboratory units for optimal sequencing of high-risk pathogens of epidemic potentials. As stressed before, adequate community education and engagement, early detection, adequate case management, and disinfection remain the mainstay of de-escalating MVD outbreaks. These containment modalities seem adequate but more has to be done about discovering vaccines for MVD. Likewise, in EVD management, these strategies could be deployed synergistically with an effectual vaccine against the Marburg virus shortly to mitigate MVD epidemics in sub-Saharan Africa.
References
- WHO Marburg virus fact sheet. 2025. https://www.who.int/news-room/fact-sheets/detail/marburg-virus-disease
- Reuters. Suspected outbreak of Marburg virus kills eight in Tanzania, WHO says. 2025. https://www.reuters.com/world/africa/suspected-outbreak-marburg-virus-kills-eight-tanzania-who-says-2025-01-15/
- WHO News. 2022. https://www.who.int/news/item/21-11-2022-who-to-identify-pathogens-that-could-cause-future-outbreaks-and-pandemics
- Kortepeter MG, Dierberg K, Shenoy ES, Cieslak TJ. Marburg virus disease: a summary for clinicians. Int J Infect Dis. 2020; 99: 233‐242.
- Brauburger K, Hume AJ, Mühlberger E, Olejnik J. Forty‐five years of Marburg virus research. Viruses. 2012; 4: 1878‐1927.
- Okonji OC, Okonji EF, Mohanan P, et al. Marburg virus disease outbreak amidst COVID‐19 in the Republic of Guinea: a point of contention for the fragile health system. Clin Epidemiol Global Health. 2022; 13: 100920.
- Ahmed I, Salsabil L, Hossain MJ, Shahriar M, Bhuiyan MA, Islam MR. The recent outbreaks of Marburg virus disease in African countries is indicating potential threat to the global public health: future prediction from historical data. Health Sci Rep. 2023; 6: e1395.
- Okonji OC, Okonji EF, Mohanan P, et al. Marburg virus disease outbreak amidst COVID‐19 in the Republic of Guinea: a point of contention for the fragile health system. Clin Epidemiol Global Health. 2022; 13: 100920.
- Towner JS, Amman BR, Sealy TK, et al. Isolation of genetically diverse Marburg viruses from Egyptian fruit bats. PLoS Pathog. 2009; 5: e1000536.
- Relief Web. DR Congo. The (new) M23 offensive on Goma: Why this long-lasting conflict is not only about minerals and what are its implications?. 2025. https://reliefweb.int/report/democratic-republic-congo/new-m23-offensive-goma-why-long-lasting-conflict-not-only-about-minerals-and-what-are-its-implications-qa
- Africa Center for Strategic Studies. Risk of Regional Conflict Following Fall of Goma and M23 Offensive in the DRC. 2025. https://africacenter.org/spotlight/risk-of-regional-conflict-following-fall-of-goma-and-m23-offensive-in-the-drc/
- Sohan Md, Shahriah M, Bhuiyan MA, Islam Md. Recent outbreak of Marburg virus disease: Could it be a threat for global public health?. Health Sci Report. 2022.
- Srivastava S, Sharma D, Kumar S, Sharma A, Rijal R, Asija A. et al. Emergence of Marburg virus: a global perspective on fatal outbreaks and clinical challenges. Frontiers in Microbiology. 2023.
- Hussain Z. Ghana declares its first outbreak of Marburg virus disease after two deaths. BMJ. 2022; 378: o1797.
- Schuh AJ, Amman BR, Jones MEB, Sealy TK, Uebelhoer LS, Spengler JR et al. Modelling filovirus maintenance in nature by experimental transmission of Marburg virus between Egyptian roussette bats. Nat Commun. 2017; 8: 14446.
- Amman BR, Carroll SA, Reed ZD, Sealy TK, Balinandi S, Swanepoel R et al. Seasonal pulses of Marburg virus circulation in juvenile Rousettus aegyptiacus bats coincide with periods of increased risk of human infection. PLoS Pathog. 2012; 8: e1002877.
- Amman BR, Jones MEB, Sealy TK, Uebelhoer LS, Schuh AJ, Bird BH et al. Oral shedding of Marburg virus in experimentally infected Egyptian fruit bats (Rousettus aegyptiacus). J Wildl Dis. 2015; 51: 113–124.
- Schwartz DA. Maternal filovirus infection and death from Marburg and Ravnviruses: highly lethal to pregnant women and their fetuses similar to Ebola virus, in emerging challenges in filovirus infections. United Nation. IntechOpen. 2019.
- Malik S, Dhasmana A, Bora J, Uniyal P, Slama P, Preetam S et al. Ebola virus disease (EVD) outbreak re-emergence regulation in East Africa: preparedness and vaccination perspective. Int J Surg. 2023; 109: 1029–1031.
- Heeney JL. Hidden reservoirs. Nature. 2015; 527: 453–455.
- Abir MH, Rahman T, Das A, et al. Pathogenicity and virulence of Marburg virus. Virulence. 2022; 13: 609‐633.
- Nyakarahuka L, Shoemaker TR, Balinandi S, et al. Marburg virus disease outbreak in Kween district Uganda, 2017: epidemiological and laboratory findings. PLOS Negl Trop Dis. 2019; 13: e0007257.
- Sissoko D, Duraffour S, Kerber R, et al. Persistence and clearance of Ebola virus RNA from seminal fluid of Ebola virus disease survivors: a longitudinal analysis and modelling study. Lancet Glob Health. 2017; 5: e80‐e88.
- Kortepeter MG, Bausch DG, Bray M. Basic clinical and laboratory features of filoviral hemorrhagic fever. J Infect Dis. 2011; 204: S810‐S816.
- Chakraborty S, Chandran D, Mohapatra RK, Alagawany M, Yatoo MI, Islam MA, et al. Marburg virus disease–a mini-review. J Exp Biol Agric Sci. 2022; 10: 686-696.
- Islam MA, Adeiza SS, Amin MR, Kaifa FH, Lorenzo JM, Bhattacharya P, et al. A bibliometric study on Marburg virus research with prevention and control strategies. Front Trop Dis. 2023; 3: 1068364.
- Olejnik J, Mühlberger E, Hume AJ. Recent advances in Marburgvirus research. F1000Res. 2019; 8: F1000.
- Feldmann H, Sanchez A, Geisbert T. Filoviridae: Marburg and Ebola viruses. H. Feldmann 6th edn. ESP: Wolter Kluwer Health Adis; Field Virology. 2013.
- Elsheikh R, Makram AM, Selim H, Nguyen D, Le TTT, Tran VP, et al. Reemergence of Marburgvirus disease: update on current control and prevention measures and review of the literature. Rev Med Virol. 2023; 33: e2461.
- Chowdhury PPD, Haque MA, Ahamed B, Tanbir M, Islam MR. A brief report on monkeypox outbreak 2022: historical perspective and disease pathogenesis. Clin Pathol. 2022; 15: 2632010X2211316.
- Hussein MF, Saleeb AG, Tessema EM, Gaitano DO, Nathanson M, Nthabiseng Tsoeu N, et al. Knowledge, attitudes and practices of the general population towards Marburg virus disease in sub-Saharan African countries: a cross-sectional study. Transactions of The Royal Society of Tropical Medicine and Hygiene. 2024: trae122.
- Okesanya OJ, Manirambona E, Olaleke NO, Osumanu HA, Faniyi AA, Bouaddi O, et al. Rise of Marburg virus in Africa: a call for global preparedness. Ann Med Surg. 2023; 85: 5285-5290.
- Semancik CS, Cooper CL, Postler TS, Price M, Yun H, Zaric M, et al. Prevalence of human filovirus infections in sub-Saharan Africa: A systematic review and meta-analysis protocol. Syst Rev. 2024; 13: 218.
- Prunier G. Africa’s World War: Congo, The Rwandan Genocide, and the Making of a Continental Catastrophe. New York: Oxford University Press. 2009: 290-306.
- Mehedi M, Groseth A, Feldmann H, Ebihara H. Clinical Aspects of Marburg Hemorrhagic fever. Future Virol. 2011; 6: 1091-106.
- Languon S, Quaye O. Filovirus Disease Outbreaks: A Chronological Overview. Virology (Auckl). 2019.
- Asad A, Aamir A, Qureshi NE, Bhimani S, Jatoi NN, Batra S, et al. Past and Current Advances in Marburg Virus Disease: A review. Le infezioni in medicina. 2020: 332-345.
- Deb N, Roy P, Jaiswal V, Mohanty A, Sah S, Sah, R. Marburg virus disease in Tanzania: the most recent outbreak. New Microbes New Infect. 2023; 53: 101123.
- Nyakarahuka L, Shoemaker TR, Balinandi S, Chemos G, Kwesiga B, Mulei S, et al. Marburg virus disease outbreak in Kween District Uganda, 2017: epidemiological and laboratory findings. PLoS Negl Trop Dis. 2019; 13: e0007257.
- Han HJ, Wen HL, Zhou CM, Chen FF, Luo LM, Liu JW, et al. Bats as reservoirs of severe emerging infectious diseases. Virus Res. 2015; 205: 1–6.
- Randhawa N, Bird BH, VanWormer E, Sijali Z, Kilonzo C, Msigwa A, et al. Fruit bats in flight: a look into the movements of the ecologically important Eidolon helvum in Tanzania. One Health Outlook. 2020; 2: 16.
- World Health Organization. Key Facts on Ebola. 2023. https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease
- Marlin R, Desjardins D, Contreras V, Lingas G, Solas C, Roques P, et al. Antiviral efficacy of favipiravir against zika and SARS-CoV-2 viruses in non-human primates. Nat Commun. 2022; 13: 5108.
- Marzi A, Jankeel A, Menicucci A. R, Callison JO, Donnell KL, Feldmann F, et al. Single dose of a VSV-based vaccine rapidly protects macaques from Marburg virus disease. Front Immunol. 2021; 12: 774026.