
Research ArticleOpen Access, Volume 3 Issue 2
An analysis of intra-familial transmission in Chronic Hepatitis-B (CHB) infected families
Tanu Yadav; Suchit Swaroop*
Experimental and Public Health Laboratory, Department of Zoology, University of Lucknow, Lucknow, UP, India.
*Corresponding author: Suchit Swaroop
Associate Professor, Experimental and Public Health Laboratory, Department of Zoology, University of Lucknow, Lucknow, UP 226007, India.
Email: Ephlab19@gmail.com
Received : Jul 07, 2025 Accepted : Aug 25, 2025 Published : Sep 01, 2025
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Swaroop S © All rights are reserved
Citation: Yadav T, Swaroop S. An analysis of intra-familial transmission in Chronic Hepatitis-B (CHB) infected families. Epidemiol Public Health. 2025; 3(2): 1075.
Abstract
Aim: This study concentrated on the pattern of intra-familial Hepatitis-B Virus (HBV) transmission. It has been observed that the infection can also be passed to any of the family member of Chronic Hepatitis-B (CHB) infected individuals from them.
Subject and methods: Questionnaire was designed and a thorough inspection of family members of the CHB positive patients performed for further investigation.
Results: The result showed that out total of 971 family members of 124 CHB infected patients only 65 parents, 114 siblings, 18 spouses, 44 children, and 7 relatives were found infected with CHB. Family size is directly proportional to the rate of CHB infection.
Conclusion: Horizontal transmission was prevalent in this study. One way mode of transmission of HBV from mother to children i.e., perinatal transmission can be possible among few CHB infected individuals. The hepatitis-B virus infects multiple generations of the family. Therefore, standardised policies and awareness program should be formed to protect people from getting CHB infection.
Keywords: CHB; Intrafamilial transmission; Horizontal transmission; Family size.
Introduction
Hepatitis-B (HB) viral infection is a threat, causing morbidity and mortality to a large population worldwide [1]. Among various Hepatitis variants only a few are generally diagnosed in Asian countries, such as A, B, C, D, E. Hepatitis-B (HB) and Hepatitis-C (HC) are the most common of all variants in east Asian countries. As per WHO report in year 2022, 254 million Chronic Hepatitis-B (CHB) infectious patients were surviving with increase of 1.2 million newer ones each year (WHO Hepatitis-B report, 9 April 2024). In India Hepatitis-B, both acute and chronic occur due to transmission of Hepatitis B Virus (HBV) which may further leads to hepatocellular carcinoma [2]. In 2019, 820000 causalities were recorded via Hepatitis-B Virus (HBV) transmission through body fluids [3].
HBV infection is primarily acute in nature and turns chronic after longer duration of infection [4], i.e., HBsAg seropositivity at 6 months or beyond [5]. Chronic Hepatitis-B (CHB) can be transmitted via either horizontal or perinatal mode, possibly through blood or other body serum such as vaginal fluid, semen, saliva, sweat, tears, breast milk, etc [6,7]. In case of horizontal transmission, HBV can be transmitted either from one partner to other through sexual contact, mother to child or child to child through injectables or through contact in wounded region and vertical (perinatal) transmission is only possible from mother to neonate [8].
Possibility of CHB transmission among family members would be higher as they remain in close proximity to reactive patients and virus can communicate through other body fluids. Sharing food items and clothes among family members can also spread CHB [9]. Increased number of infections may lead to outburst of an endemic in the country though measures have been taken via various vaccination programs, by many public health authorities to check or reduce the rate of infection among population. Possibly high risk of infection among family members of HBV- infected patients can be observed [10], but a detailed and précised mode of transmission was not studied in Uttar Pradesh region.
There was un-availability of data regarding prevalence of intrafamilial transmission of the with CHB patients in Uttar Pradesh and so in population of Uttar Pradesh India. This uncertainty about the rate of transmission of HBV can cause higher number of CHB (HBsAg positive) patients in the community and family too. Therefore, to fill the gap this study was conducted and it had been aimed to investigate the pattern, mode, magnitude of intrafamilial transmission of HBV infection to identify the family members with highest risk. This would predict the potentiality of source transmission within the family of CHB (HBsAg positive) patients.
Materials and methods
This is a cross-sectional study based on retrospective observations of HBV indexed patients and their family members to find whether CHB patients are potential to spread infection within their family. Total of 130 respondents have been selected for the study but due to incomplete data of the family of 06 patients were excluded from our study hence only 124 patients were included for data sampling and further study. All respondents gave their consent to complete the questionnaire.
This study was designed on the basis of HBsAg positivity and measures of viral load in CHB patients and carried out at OPD of the Department of Medicine of KGMU, Lucknow, Uttar Pradesh. HBsAg status of family members (who were in co-habitation with the infected CHB patient) was verified both either from the self-report of patient or laboratory reports of the close contacts with the patient. The study was carried out on the data of patients attending the clinic for the duration from November 2022 to June 2023. King George Medical University’s institutional ethics committee approved the study (1870/Ethics/2023) on 12/01/2023.
Study sample
All CHB (HBsAg positive) patients referred to the OPD of Department of Medicine were included in the study. Those individuals who were not ready to give consent for the study were excluded. CHB patients along with their family members were enrolled in the study for further analysis. The participants either themselves or their guardians in the case of minor participants, had given their consent to become an active participant in the study.
Family tree was prepared by interviewing the CHB patients and their family members. The interview included risk factors (tattoo, any surgery, and sharing of households and clothes). Total number of CHB (HBsAg positive) patients and total number of family members were calculated. Demographic distribution of study sample, distribution according to HBsAg status (reactive versus non-reactive) and relationship with the CHB patients (parents, siblings, grandparents etc). Detailed segregation of study sample according to HBsAg status and relationship with the CHB patient (mother, father, brother, sister, son, daughter etc.) was studied.
Data collection (Sampling)
Data were collected on a predesigned proforma which involved genealogical analysis of family members showing HBsAg reactivity. The family tree of each patient was studied carefully.
The family members were segregated based on the type of transmission either horizontal (spread of virus through non-sexual, non-hereditary contact with an infected person i.e., transmission occurs via household) or vertical (transmission from an infected mother to her child during pregnancy or childbirth. Vaccinated family members were considered normal individual in this study.
No CHB patient undergoing antiviral treatment was excluded in this study.
Data analysis
Data was recorded separately for male and female CHB reactive patients and their family members. Segregated list of HBsAg-positive and HBsAg-negative family members was prepared. Taking into consideration that each individual acts as a source of transmission therefore data was recorded separately. Data recorded as ‘1’ for all the HBsAg-positive family member and ‘0’ for HBsAg-negative family member. The categories were distributed in such a manner as infected father, infected mother and both. This method of data collection was applied to other family members as well. The population was differentiated into horizontally and vertically transmitted.
Statistical Analysis has been done on SPSS 20 version. Chi square test was applied to test whether there is any significant association between CHB patients and their family. The Hypothesis states that there is no association between CHB infection in indexed patients and their family members.
Results
This study was performed on a total of 130 CHB patients, and their CHB infected and CHB non-infected family members were also analysed to study intrafamilial transmission. 06 subjects were excluded from the study because they provided insufficient data. So, the total number of subjects included in the study was 124. The demographic distribution of subjects enrolled entails a total of 124 CHB patients out of which there were 84 males and 40 females. All 124 CHB patients, had an average age of 37 (±13.48). The minimum age of the CHB patient enrolled in the present study was 15 years, while the maximum age reported was 64 years. In the case of 84 (67.74%) CHB positive males, the average age was 39 years (±13.94), while in case of 40 (32.25%) female CHB active patients, the average age was 35 years (±12.16).
A total of 971 family members of 124 CHB positive patients were also analysed. There were 248 CHB positive family members of CHB infected patients reported in the study, which encompassed 65 parents, 114 siblings, 18 spouses, 44 children, and 7 relatives including maternal and paternal uncles and aunts, grandparents, cousins/others. No data was analysed further for HBsAg negative family members.
In this study, segregation of CHB positive family members in consonance with relatedness to CHB patients was done. A total of 65 CHB infected parents were reported in this study. Among the family members of male CHB infected individuals (enrolled CHB patients in the present study), 21 HBV infected father, and 21 infected mothers was reported.
Among female CHB infected individuals (enrolled CHB patients in the present study) had received 04 HBV infected father, 15 CHB infected mothers were reported. Only 3 CHB infected families where both parents (father+ Mother) of male CHB patients and 1 family of the female CHB infected patients were reported (Figure 1). A statistically significant p value of 0.092 was obtained for the association between parents and CHB infected patients. So, the parents of enrolled CHB infected patients may have been a potential mode of transmission.
Out of total family members, the highest number of members reported in the study were siblings (114) of the CHB infected patients. Among all male CHB infected individuals (enrolled CHB patients in the present study), 38 male HBV infected siblings(brothers) and 11 female CHB infected siblings (sisters) were reported. Moreover, of the total female CHB infected individuals (enrolled CHB patients in the present study), 12 male HBV infected siblings (brother), and 17 female CHB infected siblings (sisters) were reported.
Whereas siblings (brother and sister) of 25 male siblings (enrolled CHB patients in the present study) and 11 female siblings had received HBV infection from either of their CHB infected siblings (infected brother and sister). A p value of 0.004 was obtained, for the association between siblings and CHB infected patients (Figure 2). So, the enrolled CHB infected siblings may have higher potential of HBV transmission from/to their siblings.
Out of the total of 44 HBV infected offspring (children of the CHB infected patients) enrolled in the study, only 12 male children (sons) HBV infected of female CHB patients and 10 male children of male CHB infected parents were reported. Whereas, 7 female children (daughters) of male CHB patients and 6 female children of female CHB patients were reported. Whereas, 4 children (both daughter and son/all children) of CHB positive male patients and 5 children (both daughters and son/ all children) of CHB positive female patients were reported. A p value of 0.92 was obtained against CHB patients and their offspring (Figure 3).
In this study, CHB positive patients among spouses was 18 in number, either male, or female and both partners were found infected.
Male CHB patients whose wives were also found infected with hepatitis-B virus were 11 in number. While female CHB patients whose husband found CHB infected were 7 in number. A p value of 0.00 was obtained that was significantly less than standard p value of 0.05 for association between CHB infected spouses (Figure 4).
The family members other than closely related (Father, mother, siblings, spouses) such as grandparents, paternal uncles, maternal uncles were reported to be very less in number and tabulated in this study (Table 1). No association between those relatives and CHB positive patients was obtained due to the limited data acquired in this study.
This study also focused on whether the size of the family has some effect on the transmission of CHB infection within the family. The family size was categorised into three categories: in the first category, the members within the family were less than 4. In the second category, there are only four members in a family and in the third category, there are more than four members in the family (Figure 5).
The families were further categorised into nuclear and joint based on the number of children and other related members living together at the same dwelling place. A nuclear family here includes parents and their children only, irrespective of the number of children within the family. The number of children may vary from one to numerous in the nuclear family in this study. Though a joint family has other family members living together, such as a paternal uncle, a paternal aunt, or maternal relatives, a higher percentage of nuclear families was reported (Figure 6).
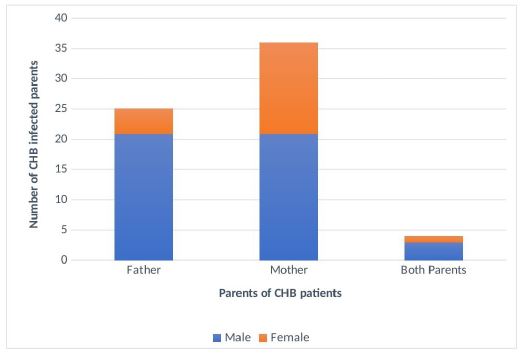
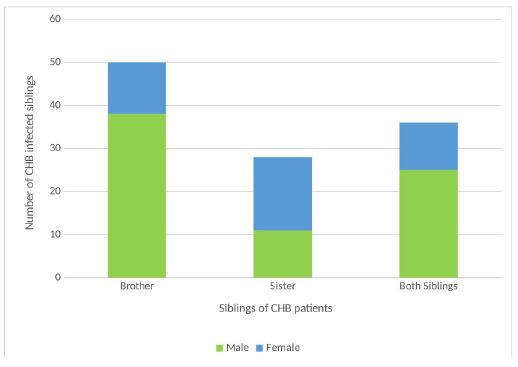
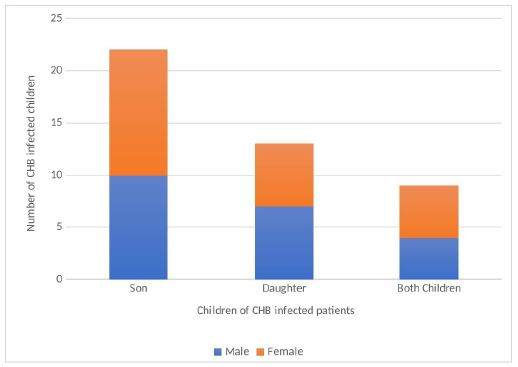
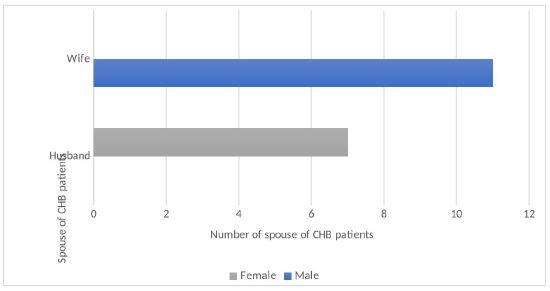
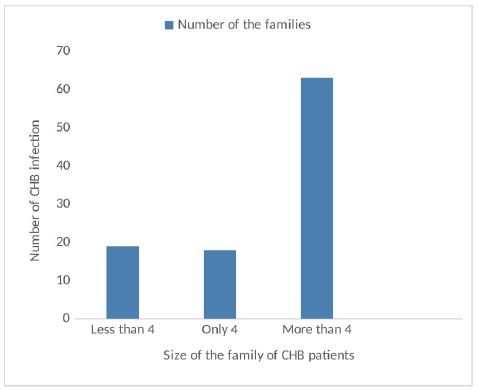
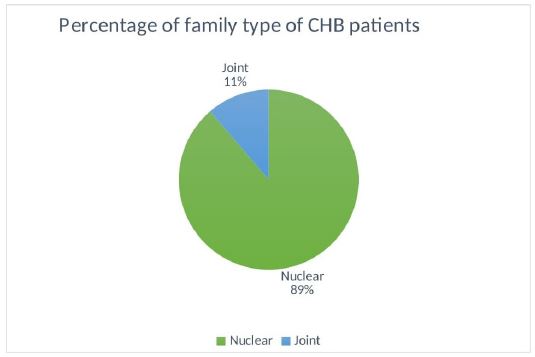
Table 1: Frontal CT scan showing the mass an upper polar tissue mass of the left kidney.
| Miscellaneous | Male | Female | Total |
|---|---|---|---|
| Grand father | 2 | - | 2 |
| Grand mother | 2 | - | 2 |
| Maternal uncle | 1 | - | 1 |
| Paternal uncle | 2 | - | 2 |
Discussion
In India, hepatitis-B onset and its development cannot be specified for a particular age group; rather, its progression was observed at all ages. Therefore, it is necessary to understand the transmission of the hepatophilic infection by HBV. In this study, transmission of HBV within the family has been reported in only 26.89% of the total family members enrolled in this study, i.e., 989, of 124 CHB positive patients (sample population). It has been observed in this study that horizontal transmission among siblings of no specific age has a higher rate in familial relationships than any other closed family member, similar to another study performed over children under 15 years of age among the Uttar Pradesh population [9].
The HBV transmission rate from infected CHB parents is higher in males than females. A p value of 0.44 was obtained, which is higher than standard p value 0.05; hence, we accept the hypothesis and conclude that HBV transmission in CHB infected patients has no significant association with the CHB infected parents.
The prevalence of offspring infected with CHB in the Uttar Pradesh population, was only 11.82 percent of the total HBV infected population (CHB positive patients and their family members, i.e., 248+124=372). For the association between CHB patients and their children, a p value of 1.0 was obtained, which is greater than 0.05; hence, there was no statistically significant association observed between offspring and their CHB infected parents. Majorly, HBV transmission from mother to child via perinatal mode is higher than the paternal transmission reported by [11]; similarly, in this study, it was also reported that the percentage of HBV transmission from mothers to their children is higher (1.95%) than the HBV transmission from father to offspring (1.43%).
A p value of 0.00 was obtained which is less than standard 0.05 value of p, for the partners of CHB patients and them. Therefore, the null hypothesis was rejected, and hence it can be inferred that there was an association between the transmission of CHB patients and their spouses in this study. According to a previous study performed by [12] HBV exposed partners showed associations with the transmission of HBV to other partners; transmission of HBV from a CHB infected patient to their spouse was significant in this study. In this study, it was also reported that HBV transmission from spouse to spouse was lower than transmission from sibling to sibling and from parents to child but higher than that observed among other family members (grandparents, maternal, and paternal relatives).
The risk of HBV transmission other than that of siblings, was lower among family members of CHB patients.
Most mothers were transmitting the virus to the children rather than any other family member, but it is imprecise to say that the transmission of the HB virus occurred via perinatal mode. Therefore, it can be concluded that HBV transmission in Uttar Pradesh, among siblings is higher and horizontal transmission has proven more prevalent than perinatal transmission. This data unlikely to an earlier study performed in west India on members of a single family by [13].
Though the occult spread of HBV infection was not determined in our study, HBV transmission via oral, mucosal, or cutaneous contacts may be possible with infected family members. Sharing of personal objects, for instance, clothes, bath towels, eating and drinking utensils, toothbrushes, nail clippers, etc., was considered an important factor in HBV transmission in earlier studies. In Ghana and Brazilian studies, toothpaste, bathing towels, chewing gum were found to be significantly associated with the prevalence of CHB positivity within families [13].
Conclusion
It can be concluded that there can be transmission of Hepatitis-B virus among the family members can be possible because of the high number of offspring and siblings who were in close vicinity to the infected CHB patients. Higher significance of transmission possibility had been noticed between sibling to sibling and from mother to their children. Hence, it can be said that horizontal transmission is prevalent among people of Uttar Pradesh.
Transmission within the family as per family size was not focused, but a higher number of patients reported from families with more than four family members. This result may lead to a conclusion that families with a higher number of members who shared their daily household items, have higher chances of HBV transmission within the family. Families living in close proximity to the HBV infected person have higher chances of transmission.
The potential for source transmission from a CHB positive subject within a family has been calculated in this study. This would help in determining the spread and probability of transmission within the CHB infected family.
Transmission of viruses from parents to children via perinatal transmission can be possible. The uninvestigated premarital status of individuals was a limitation of this study. The hepatitis-B virus infects multiple generations of the family. Proper measures to prevent intra-familial transmission should be recommended.
Declarations
Acknowledgement: We thank Professor. Sangeeta Rani (Head of the Department), Department of Zoology, University of Lucknow) for conduction of research work in the Department of Zoology. We thank King George’s Medical College authority for permitting the data collection. We also show our gratitude towards Dr. Ajay Kumar Patwa (Professor, Department of Medicine) for his support and guidance in collecting data. Dr. Shambhavi Mishra (Assistant Professor, Department of Statistics, University of Lucknow) for her assistance in statistical analysis.
Funding: No Funding agency was involved in the study/ not applicable.
References
- Kheir OO, et al. Assessment of hepatitis B knowledge and awareness among the Sudanese population in Khartoum State. Pan Afr Med J. 2022; 41: 1–8.
- Chakravarty R, Chowdhury A, Chaudhuri S, Santra A, Neogi M. Hepatitis B infection in Eastern Indian families: need for screening of adult siblings and mothers of adult index cases. Public Health. 2005; 119: 647–654.
- Sonkar A, Bishwal SC, Sharma RK, Barde PV. Prevalence of hepatitis D virus antibodies in hepatitis B patients treated at tertiary care unit at Jabalpur, Central India. Indian J Med Microbiol. 2022; 40: 132–134.
- Guvenir M, Arikan A. Hepatitis B virus: from diagnosis to treatment. Mikrobiyol Bul. 2020; 69: 391–399.
- Sarin SK, Kumar M, Lau GK, Abbas Z, Chan HL, Chen CJ, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016; 10: 1–98.
- MacLachlan JH, Cowie BC. Hepatitis B virus epidemiology. Cold Spring Harb Perspect Med. 2015; 5: a021410.
- Athalye S, Tiwari A, Singh A, Deshpande P, Verma R, Gupta S, et al. Exploring risk factors and transmission dynamics of hepatitis B infection among Indian families: implications and perspective. J Infect Public Health. 2023; 16: 1109–1114.
- Nguyen MH, Wong G, Gane E, Kao JH, Dusheiko G. Hepatitis B virus: advances in prevention, diagnosis, and therapy. Clin Microbiol Rev. 2020; 33: e00046-19.
- Joshi YK, Singh S. Role of horizontal transmission in hepatitis B virus spread among household contacts in North India. Dig Dis. 2008; 26: 106–112.
- Urganci N, Akyildiz BN, Kalyoncu D, Gulec SG. Familial clustering of HBV in families with children who are diagnosed as chronic hepatitis B or inactive carriers of HBV. J Child Health Care. 2013; 17: 197–203.
- Yang Y, Li X, Zhang W, Chen Y, Zhao L, Sun H, et al. The association of adverse outcomes in the mother with disease progression in offspring in families with clusters of hepatitis B virus infection and unfavorable prognoses in Northwest China. J Viral Hepat. 2020; 27: 281–288.
- Zhao X, Lv M. Prevalence and factors associated with hepatitis B virus infection among household members: a cross-sectional study in Beijing. Hum Vaccin Immunother. 2021; 17: 1818–1824.
- Debnath P, Bhowmik S, Roy S, Sarkar A, Mandal P, Saha P, et al. Familial transmission of hepatitis B: an interesting case report. Int J Community Med Public Health. 2020; 7: 3693–3696.