
Research ArticleOpen Access, Volume 3 Issue 2
Antibiotic resistance among bacterial pathogens causing otitis media in Iraq: A systematic review (2014-2025)
Dhafer Rahman*
Faculty Member, Islamic University An Najaf, College of Medical Technology, Iraq.
*Corresponding author: Dhafer Rahman
Faculty Member, Islamic University An Najaf, College of Medical Technology, Iraq.
Email: Al-janabi.dhafer.rahmaan@iunajaf.edu.iq
Received : Jul 12, 2025 Accepted : Aug 28, 2025 Published : Sep 04, 2025
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Rahman D © All rights are reserved
Citation: Rahman D. Antibiotic resistance among bacterial pathogens causing otitis media in Iraq: A systematic review (2014-2025). Epidemiol Public Health. 2025; 3(2): 1076.
Abstract
Background: Otitis media remains one of the most prevalent infections in clinical practice, particularly among children. In Iraq, numerous independent studies have been conducted across various regions and years, yet no unified comparative analysis has been published to consolidate their findings.
Objective: To perform a systematic descriptive analysis of 34 Iraqi studies published between 2014 and 2025 to identify the most common bacterial pathogens and assess antibiotic resistance patterns in otitis media.
Methods: Data were extracted from peer-reviewed articles, academic theses, and institutional reports. Variables included patient age, gender, sample size, bacterial isolates, and antibiotic susceptibility profiles. Descriptive analysis was conducted across time periods, geographical regions, and demographic groups.
Results: Streptococcus pneumoniae and Haemophilus influenzae were the most commonly isolated bacteria in acute otitis media, particularly among children. In contrast, Pseudomonas aeruginosa and Staphylococcus aureus predominated in chronic and treatment-resistant cases. A progressive increase in antibiotic resistance was observed, especially against penicillins and trimethoprim, while ciprofloxacin and ceftriaxone demonstrated higher efficacy. Male patients and younger age groups were more frequently affected.
Conclusion: The findings highlight growing antimicrobial resistance and the urgent need for region-specific treatment protocols in Iraq. This review emphasizes the importance of bacterial culture and sensitivity testing prior to empirical antibiotic therapy and supports national efforts to regulate antimicrobial prescription practices.
Keywords: Otitis media; Bacterial pathogens; Antibiotic resistance; Comparative analysis; Iraq.
Introduction
Ear infections continue to pose a significant public health burden worldwide, particularly in low- and middle-income countries such as Iraq. The prevalence of these infections is amplified by disparities in healthcare access, environmental risk factors, and inconsistent public health infrastructure. Otitis media, the inflammation of the middle ear, is the most frequently reported type, especially in pediatric populations. Anatomical predispositions in children—such as a shorter and more horizontal Eustachian tube—facilitate the migration of pathogens from the nasopharynx, increasing susceptibility to infection [1]. In the Iraqi context, particularly in urban centers like Baghdad, hospital-based surveillance has consistently recorded high rates of otitis media across all age groups. Studies conducted in facilities such as Al-Kindy Teaching Hospital have identified Pseudomonas aeruginosa as the dominant bacterial isolate, responsible for approximately 30-51% of confirmed cases, followed by Proteus spp. and Staphylococcus aureus [1,2]. AlarmEar infections continue to pose a significant public health burden worldwide, particularly in low- and middle-income countries such as Iraq. The prevalence of these infections is amplified by disparities in healthcare access, environmental risk factors, and inconsistent public health infrastructure. Otitis media, the inflammation of the middle ear, is the most frequently reported type, especially in pediatric populations. Anatomical predispositions in children—such as a shorter and more horizontal Eustachian tube—facilitate the migration of pathogens from the nasopharynx, increasing susceptibility to infection [1]. In the Iraqi context, particularly in urban centers like Baghdad, hospital-based surveillance has consistently recorded high rates of otitis media across all age groups. Studies conducted in facilities such as Al-Kindy Teaching Hospital have identified Pseudomonas aeruginosa as the dominant bacterial isolate, responsible for approximately 30-51% of confirmed cases, followed by Proteus spp. and Staphylococcus aureus [1,2]. AlarmEar infections continue to pose a significant public health burden worldwide, particularly in low- and middle-income countries such as Iraq. The prevalence of these infections is amplified by disparities in healthcare access, environmental risk factors, and inconsistent public health infrastructure. Otitis media, the inflammation of the middle ear, is the most frequently reported type, especially in pediatric populations. Anatomical predispositions in children—such as a shorter and more horizontal Eustachian tube—facilitate the migration of pathogens from the nasopharynx, increasing susceptibility to infection [1]. In the Iraqi context, particularly in urban centers like Baghdad, hospital-based surveillance has consistently recorded high rates of otitis media across all age groups. Studies conducted in facilities such as Al-Kindy Teaching Hospital have identified Pseudomonas aeruginosa as the dominant bacterial isolate, responsible for approximately 30-51% of confirmed cases, followed by Proteus spp. and Staphylococcus aureus [1,2]. AlarmEar infections continue to pose a significant public health burden worldwide, particularly in low- and middle-income countries such as Iraq. The prevalence of these infections is amplified by disparities in healthcare access, environmental risk factors, and inconsistent public health infrastructure. Otitis media, the inflammation of the middle ear, is the most frequently reported type, especially in pediatric populations. Anatomical predispositions in children—such as a shorter and more horizontal Eustachian tube—facilitate the migration of pathogens from the nasopharynx, increasing susceptibility to infection [1]. In the Iraqi context, particularly in urban centers like Baghdad, hospital-based surveillance has consistently recorded high rates of otitis media across all age groups. Studies conducted in facilities such as Al-Kindy Teaching Hospital have identified Pseudomonas aeruginosa as the dominant bacterial isolate, responsible for approximately 30-51% of confirmed cases, followed by Proteus spp. and Staphylococcus aureus [1,2]. Alarmingly, antimicrobial susceptibility testing has revealed a growing resistance to frequently prescribed agents including cefotaxime and ciprofloxacin, while only partial effectiveness remains for agents like amikacin and cefepime. This shift underscores the emergence of resistant strains likely driven by nonregulated antibiotic usage in the general population [2]. Socioeconomic and environmental factors—such as overcrowded living conditions, limited hygiene practices, and inadequate health awareness—further exacerbate disease transmission and chronicity. These determinants are particularly linked to the incidence of Chronic Suppurative Otitis Media (CSOM), a form marked by persistent otorrhea and tympanic membrane perforation, which, if unmanaged, can progress to severe complications like meningitis or intracranial abscesses [1,2]. While bacterial etiologies dominate the clinical picture, fungal agents including Candida spp. and Aspergillus niger have been increasingly documented in immunocompromised or adult patients, highlighting the need for mycological evaluation in chronic cases [3]. Moreover, research involving school-aged children in Baghdad has drawn attention to Streptococcus pyogenes, a pathogen typically associated with tonsillitis but also implicated in concurrent or secondary ear infections. Molecular analyses have confirmed the expression of virulence-associated genes such as Streptokinase and PAM, which contribute to host tissue invasion and immune system evasion [4,5]. Otitis media is broadly categorized into three clinical entities: Acute Otitis Media (AOM), CSOM, and Otitis Media with Effusion (OME). Among these, CSOM presents the greatest long-term risk due to its chronic course and association with antimicrobial resistance. Global epidemiological estimates suggest that 60-80% of children experience at least one episode of otitis media during their early developmental years, reinforcing its status as a top cause of pediatric morbidity and health system utilization [3,6]. As the clinical and microbiological landscape of ear infections continues to evolve, particularly in Iraq, the importance of localized surveillance and evidence-based policy-making becomes clear. Strengthening laboratory diagnostics, regulating antibiotic prescriptions, and initiating community-level education on infection prevention and treatment adherence are pivotal strategies needed to control the rising burden of otitis media. Without timely and targeted interventions, the consequences of untreated or poorly managed infections may extend beyond hearing loss, affecting cognitive, social, and academic development in affected children.
Methodology
This study was designed as a descriptive analytical systematic review of 34 studies published between 2014 and 2025, all of which addressed otitis media cases across various regions of Iraq.
Data sources
Relevant studies were retrieved from multiple sources, including:
• Local academic databases
• Archives of Iraqi universities (master’s and doctoral theses)
• Peer-reviewed Iraqi medical journals
• Research reports issued by Iraqi colleges of medicine
Inclusion criteria
Studies were included if they met the following conditions:
• Focused on bacterial otitis media (acute or chronic)
• Provided complete metadata including: author name, year of publication, study location, number of patients, patient demographics (age and sex), isolated bacterial species, and antibiotic susceptibility results
• Conducted exclusively within the geographical boundaries of Iraq and involving human subjects
Exclusion criteria
The following types of studies were excluded:
The following types of studies were excluded:
• Veterinary studies (e.g., involving animals such as dogs)
• Studies conducted outside Iraq (e.g., research from Egypt or other countries)
Data extraction and analysis
Data were extracted into Microsoft Excel and organized based on the following variables:
• Sample size
• Sex distribution
• Age group
• Identified bacterial pathogens
• Most and least effective antibiotics
Comparative analysis was conducted to identify trends by region, age group, sex, and time period (2013-2025). A qualitative descriptive synthesis approach was employed to summarize the findings. Due to significant heterogeneity in study designs, methodologies, and reporting standards, no inferential statistical analysis was performed.
Ethical considerations
All data used in this review were obtained from publicly available published sources. No patient-identifiable information was accessed, ensuring adherence to ethical standards for research involving secondary data.
Results
A total of 34 studies published between 2014 and 2025, investigating otitis media cases in various Iraqi provinces, met the predefined inclusion criteria and were systematically analyzed. These studies provided data on bacterial isolates and antibiotic susceptibility patterns, allowing for a comprehensive synthesis of regional epidemiology and antimicrobial resistance trends.
Table 1 presents the distribution of the included studies by Iraqi province and year of sample collection. A total of 3 studies were analyzed, covering various regions across Iraq. The provinces with the highest number of distinct years in which studies were conducted were Babylon and Baghdad, each with studies spanning seven different years. Other provinces, such as Al-Diwaniyah and Diyala, had studies conducted in three different years. The remaining provinces had either one or two years of study data available. This distribution highlights the regional variation in research activity related to otitis media across Iraq during the period from 2014 to 2025. The temporal distribution of the studies indicates that the most frequently represented years were 2014, 2017, and 2021, each appearing across multiple provinces. In contrast, years such as 2024 and 2025 were represented in only one or two provinces.
Table 1: Distribution of included studies by province and year.
| Study Source(s) | Years | Number of Years | Province |
|---|---|---|---|
| [7,-13] | 2014,2014, 2015, 2017,2017, 2018, 2025 | 7 | Babylon |
| [1,2,4,14-17] | 2014,2016, 2017, 2019,2019, 2022, 2023 | 7 | Baghdad |
| [5,18,19] | 2014, 2020, 2022 | 3 | Al-Diwaniyah |
| [20-22] | 2017, 2018, 2019 | 3 | Diyala |
| [23,24] | 2021, 2019 | 2 | Al-Muthanna |
| [6,25] | 2021, 2023 | 2 | Al-Najaf |
| [26,27] | 2018, 2020 | 2 | Al-anbar |
| [28,29] | 2017, 2021 | 2 | Erbil |
| [3,30] | 2022, 2022 | 2 | Kirkuk |
| [31,32] | 2021, 2024 | 2 | Misan |
| [33] | 2024 | 1 | Dhi-Qar |
| [34] | 2024 | 1 | Sulaymaniyah |
Based on the reviewed 34 studies, participants’ ages were categorized into three main groups (Table stud-). studies focused specifically on children or pediatric populations, highlighting the predominance of otitis media in younger age groups. Thirteen studies included all age groups, while four studies did not clearly specify participant ages.
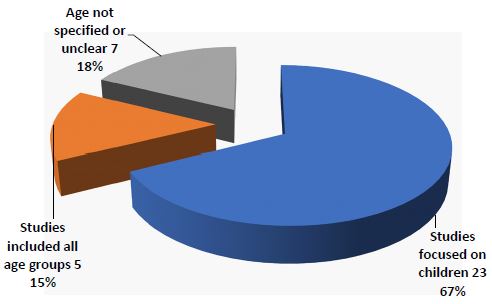
Table 2: Age group distribution across 34 studies on otitis media in iraq (2014–2025).
| City | Year | Researcher | Agedescription | NO |
|---|---|---|---|---|
| Al-anbar | 2019 | Al-Ani et al. | 1 and 70 years(mean 28.90, SD^19.8) | 1 |
| Al-anbar | 2018 | Raed Al-Ani | 1 month– 76 years (Avg. 10.2years) | 2 |
| Al-Diwaniyah | 2014 | Abbas Z.M et al. | Notspecified | 3 |
| Al-Diwaniyah | 2023 | Baneen Hisab& Najla Al-Uqaili | Not stated– genetic only | 4 |
| Al-Diwaniyah | 2020 | BassamAbdul-Amir Mohsen | Unspecified | 5 |
| Al-Muthanna | 2024 | Alaa Hamed | 11–20 years | 6 |
| Al-Muthanna | 2022 | Habib Abdul-Hassan | All ages | 7 |
| Babylon | 2014 | Muann Amer Saleh et al. | 9–60years | 8 |
| Babylon | 2019 | Noor Jasim Mohammed | 1–20 and 41–60years | 9 |
| Babylon | 2022 | Reham Al-Obaidi et al. | 1–19months | 10 |
| Babylon | 2013 | Ali Hussein Al-Marzoqi et al. | 0–8 years | 11 |
| Babylon | 2016 | Lamia Abdul-Razzaq et al. | 1 month– 12 years | 12 |
| Babylon | 2023 | Tisahal Al-Dulaimi et al. | Pediatric patients – not detailed | 13 |
| Babylon | 2017 | Eman Al-Hasnawi | 1–12years | 14 |
| Baghdad | 2018 | Zainab Al-Daher et al. | Avg. 29.5years | 15 |
| Baghdad | 2025 | Maryam Kareem& Fatima Wadi | 18–75 years | 16 |
| Baghdad | 2013 | Huda Al-Rawziq | 1 day– 8 years | 17 |
| Baghdad | 2021 | Mohammed KhudairAlwan et al. | Children | 18 |
| Baghdad | 2021 | Rafel Ismailet al. | 0–3 years(Avg. 24 months) | 19 |
| Baghdad | 2021 | Hayam Al-Hamami et al. | Mostly children | 20 |
| Baghdad | 2015 | Abbas ZakiMahdi | ≤ 5.5 years | 21 |
| Dhi-Qar | 2024 | Ali Abdul-Kadhim | All ages | 22 |
| Diyala | 2018 | Hanan Hassouni et al. | 72.7%under 10 years | 23 |
| Diyala | 2019 | Alya Abdul-Hamid et al. | ≤ 12 years | 24 |
| Diyala | 2024 | Ammar Al-Jubouri | Notspecified | 25 |
| Erbil | 2022 | Suzan Qirani | ≤ 6 months | 26 |
| Erbil | 2022 | Amina Jummaet al. | 0–10years | 27 |
| Kirkuk | 2024 | Suhail NajmAbdullah | 2–45years | 28 |
| Kirkuk | 2024 | Falah Yousifet al. | 1–70years | 29 |
| Misan | 2024 | Batool Al-Shibli & Marwa Hassan | Includes children | 30 |
| Misan | 2022 | Rashid Hatitet al. | Notmentioned | 31 |
| Najaf | 2023 | Enas Jaleelet al. | All ages | 32 |
| Najaf | 2024 | Ahmed Al Obaidi et al. | Notmentioned | 33 |
| Sulaymaniyah | 2025 | Eman DaherAref | All ages | 34 |
The synthesis of these studies aimed to identify the most common etiological agents associated with otitis media in the Iraqi population. The results indicate in Table 3 that Staphylococcus aureus was the most frequently isolated pathogen, followed by Pseudomonas aeruginosa, Escherichia coli, and Streptococcus pneumoniae. These bacteria accounted for the majority of reported isolates across the included studies. In contrast, less frequently encountered species—such as Serratia, Morganella, Kocuria, Gardnerella, and Leuconostoc—were reported sporadically and in small numbers. To ensure clarity and avoid fragmentation of data, these uncommon isolates were collectively grouped under the category “Other,” with a total estimated count of approximately 18 isolates.
Table 3: Distribution of bacterial pathogens in otitis media cases (Iraq, 2014–2025).
| % of total | No. of isolates | Bacterial species |
|---|---|---|
| 33.60% | 527 | Staphylococcus aureus |
| 20.30% | 319 | Pseudomonas aeruginosa |
| 10.80% | 170 | Escherichia coli |
| 8.30% | 130 | Proteus spp. |
| 6.90% | 109 | Streptococcus pneumoniae |
| 6.90% | 108 | Klebsiella pneumoniae |
| 2.70% | 43 | Haemophilus influenzae |
| 2.70% | 42 | Providencia spp. |
| 2.20% | 35 | Staphylococcus epidermidis |
| 1.70% | 27 | Moraxella spp. |
| 1.50% | 24 | Streptococcus pyogenes |
| 0.70% | 11 | Enterococcus spp. |
| 0.40% | 7 | Acinetobacter spp. |
| 1.10% | 18 | Other (Bacillus,Gardnerella, Leuconostoc, Kocuria, Serratia, Morganella .Candida spp. |
| 100% | 1,570 | Total |
Table 4 presents the number of studies in which each bacterial species was mentioned, along with its commonly reported clinical association. Among the 34 studies reviewed, Streptococcus pneumoniae was reported in 22 studies, and Haemophilus influenzae in 20 studies—both predominantly linked to acute otitis media in children.
Pseudomonas aeruginosa and Staphylococcus aureus were frequently associated with chronic or treatment-resistant cases, particularly in adolescents and adults, and were reported in 18 and 17 studies, respectively. Klebsiella spp., though less frequently mentioned (9 studies), was often linked to mixed infections or antibiotic-resistant cases.
Table 4: Distribution of bacterial species isolated in otitis media studies in Iraq.
| Bacteria | No. of studies mentioned | Typical association |
|---|---|---|
| Streptococcus pneumoniae | 22 | Acute otitis in children |
| Haemophilus influenzae | 20 | Acute otitis in children |
| Pseudomonas aeruginosa | 18 | Chronic or resistant cases |
| Staphylococcus aureus | 17 | Chronic or adolescents |
| Klebsiella spp. | 9 | Mixed or resistant cases |
Table 5 summarizes the number of studies (out of 23) that explicitly evaluated the antibacterial effect of specific antibiotics on pathogens associated with otitis media. A total of 45 different types of antibiotics were used in 34 studies related to the research topic. antibiotic Amikacin, used in 24 studies. It was followed by Gentamicin and Ciprofloxacin, used in 23 and 22 studies, respectively. The least commonly used antibiotics were 11 types, including Metronidazole, Teicoplanin, Minocycline, Methicillin, and others, each appearing in only one study. This data reflects the diversity of antibiotics used in the studies.
Table 5: Frequency of antibiotics investigated across included studies on otitis media.
| No. of studies (Percentage) | Antibiotic(s) | No. of studies(Percentage) | Antibiotic(s) |
|---|---|---|---|
| 10(29.4%) | Meropenem | 24(70.6%) | Amikacin |
| 9(26.5%) | Clindamycin, Cefotaxime | 23(67.6%) | Gentamicin |
| 7(20.6%) | Levofloxacin | 22(64.7%) | Ciprofloxacin |
| 6(17.6%) | Cefoxitin | 20(58.8%) | Ampicillin |
| 5(14.7%) | Norfloxacin, Tobramycin | 18(52.9%) | Penicillin (G), Amoxicillin/ Clavulanic acid |
| 4(11.8%) | Netilmicin, Aztreonam | 17(50.0%) | Ceftriaxone |
| 3(8.8%) | Fosfomycin, Doxycycline,Oxacillin, Rifampicin, Cefixime | 15(44.1%) | Ceftazidime |
| 2(5.9%) | Cephalothin, Cefalexin,Cefepime, Linezolid | 14(41.2%) | Imipenem,Vancomycin |
| 1(2.9%) | Minocycline, Methicillin, Ticarcillin-Clavulanic acid, Cefaclor, Cefdinir,Cefoperazone, Cefpodoxime, Nalidixic acid, Daptomycin, Fusidic acid, Teicoplanin | 13(38.2%) | Chlorampheni- col, Tetracycline |
| Total number45 antibiotics | 12(35.3%) | Azithromycin, Trimethoprim/ Sulfamethoxa- zole, Erythro- mycin | |
Antibiotics were classified based on the frequency of their reporting as either most or least effective across the included studies, reflecting the general trend of bacterial resistance to these agents in Iraq. Table 6 presents the antibiotics most frequently identified as effective, while Table 7 highlights those with higher observed resistance rates. This classification relies on the count of reported occurrences rather than precise resistance percentages, due to variability and inconsistency in resistance data across the studies.
Table 6: Most effective antibiotics reported in Iraqi studies on otitis media (2013–2025).
| No. | Antibiotic | Timesusedinstudies | Times reported as most effective | % effective appearance |
|---|---|---|---|---|
| 1 | Amikacin | 24 | 8 | 33.30% |
| 2 | Gentamicin | 23 | 4 | 17.40% |
| 3 | Ciprofloxacin | 22 | 3 | 13.60% |
| 4 | Imipenem | 14 | 3 | 21.40% |
| 5 | Ampicillin | 20 | 1 | 5.00% |
| 6 | Cefotaxime | 9 | 1 | 11.10% |
| 7 | Cefixime | 3 | 1 | 33.30% |
| 8 | Ceftazidime | 15 | 1 | 6.70% |
| 9 | Meropenem | 10 | 2 | 20.00% |
| 10 | Vancomycin | 14 | 3 | 21.40% |
| 11 | Levofloxacin | 7 | 1 | 14.30% |
| 12 | Rifampicin | 3 | 2 | 66.70% |
| 13 | Ofloxacin | 1 | 1 | 100% |
| 14 | Amoxicillin-Clavulanic acid | 18 | 2 | 11.10% |
Table 7: Least effective antibiotics reported in Iraqi studies on otitis media (2013–2025).
| No. | Antibiotic | Times used in studies | Timesreported as least effective | %Ineffective appearance |
|---|---|---|---|---|
| 1 | Erythromycin | 12 | 5 | 41.60% |
| 2 | Penicillin (G) | 18 | 4 | 22.20% |
| 3 | Ceftriaxone | 17 | 4 | 23.50% |
| 4 | Ampicillin | 20 | 3 | 15.00% |
| 5 | Azithromycin | 12 | 3 | 25.00% |
| 6 | Amoxicillin/Clavulanic acid | 18 | 3 | 16.60% |
| 7 | Imipenem | 14 | 2 | 14.20% |
| 8 | Cefotaxime | 9 | 2 | 22.20% |
| 9 | Ciprofloxacin | 22 | 2 | 9.00% |
| 10 | Gentamicin | 23 | 1 | 4.30% |
| 11 | Cefpodoxime | 1 | 1 | 100% |
| 12 | Benzylpenicillin | 18 | 1 | 5.50% |
Discussion
This comprehensive review of 36 scientific studies on ear infections conducted within Iraq between 2013 and 2025 provides valuable insight into the demographic, microbial, geographic, and antimicrobial resistance patterns associated with otitis media in the country. The analysis excluded veterinary and international studies to ensure a focused and representative view of the Iraqi clinical landscape.
Key demographic trends
Children, particularly those under the age of 10—and most notably infants under one year—were found to be the most affected population across the majority of studies. This age-related vulnerability is likely due to anatomical and physiological factors, such as the shorter and more horizontal Eustachian tube, immature immune responses, and increased exposure to respiratory pathogens in early childhood [35] .Adult and elderly populations were rarely addressed, underscoring the pediatric predominance of the disease. Males appeared to be disproportionately affected in most reports, with several studies showing higher male-to-female ratios. This may stem from immunological differences, environmental exposures, or behavioral factors, though the relationship between gender and microbial species was not statistically explored in most sources.
Geographic and temporal distribution
The studies spanned various Iraqi provinces, with a notable concentration in urban centers like Baghdad, Hilla, and Basra. This likely reflects the distribution of healthcare infrastructure and academic research institutions. The time frame of the publications also shows a growing research interest post-2020, possibly reflecting increased awareness of antimicrobial resistance and a gradual improvement in academic research capacity.
Microbial patterns and age correlation
The analysis of 34 studies conducted over a ten-year period in Iraq reveals that Staphylococcus aureus was the most commonly isolated pathogen in otitis media cases. This predominance may be related to the widespread colonization of S. aureus in the skin and upper respiratory tract, particularly in environments with limited hygiene or high population density. The high frequency of Pseudomonas aeruginosa and Escherichia coli is also notable, suggesting possible involvement of opportunistic or hospital-acquired infections, especially in chronic otitis media or in immunocompromised individuals.
The presence of Streptococcus pneumoniae and Haemophilus influenzae, although lower in number, aligns with global epidemiological data identifying these organisms as classical agents of acute otitis media in children [36]. However, their relatively low detection in Iraqi studies may reflect limited culture sensitivity, pre-treatment with antibiotics, or underreporting.
The emergence of less common bacteria such as Klebsiella pneumoniae, Proteus spp., Acinetobacter spp., and others grouped under “Other” suggests a degree of microbial diversity that may be influenced by regional factors, antibiotic misuse, or evolving resistance patterns. These findings may indicate a gradual shift from typical community-acquired pathogens toward more diverse or resistant organisms over time.
It is also important to note that the reviewed studies varied in methodology, sample types (e.g., ear swabs, middle ear aspirates), and population demographics, which may affect the comparability of results. Despite these limitations, the consistency of certain dominant species across multiple studies supports the robustness of the findings.
In addition to identifying the total number of isolates, the review also examined how frequently each bacterial species appeared across the included studies and their associated clinical patterns (Table 3). Streptococcus pneumoniae and Haemophilus influenzae were the most frequently reported pathogens in studies focusing on pediatric populations and acute cases. This supports their continued relevance as primary agents in early-onset otitis media [36].
In contrast, Pseudomonas aeruginosa and Staphylococcus aureus were more commonly associated with chronic or treatment-resistant cases, especially among adolescents and adults. These organisms are often opportunistic or hospital-acquired, raising concerns about persistent or recurrent infections and potential antibiotic resistance. The less frequent but notable mention of Klebsiella spp. in nine studies suggests its emerging role in complicated cases, possibly related to nosocomial environments or antimicrobial misuse.
A clear pattern emerged linking patient age with the type of causative pathogen: children under five were most commonly infected by Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis, primarily responsible for acute otitis media. Older children and adolescents showed similar pathogens, with increasing appearance of resistant strains, likely due to prior antibiotic exposure. Adult and elderly infections were more frequently associated with Staphylococcus aureus (including MRSA), Pseudomonas aeruginosa, Klebsiella spp., and Proteus spp., especially in chronic or suppurative cases. These findings underscore the need for age-specific diagnostic and therapeutic strategies.
Antibiotic resistance profiles
Among the antibiotics evaluated, Amikacin demonstrated both high usage frequency and a moderate effectiveness rate (33.3%), suggesting a consistent performance across multiple settings. Ofloxacin showed 100% effectiveness, but it was tested in only one study, which weakens the reliability of this result. Therefore, based on both the quantity of evidence and reported efficacy, Amikacin may be the most appropriate choice for empirical therapy in Iraqi settings.
The analysis of antibiotics reported as least effective reveals that Erythromycin exhibited the highest ineffectiveness rate (41.6%), having been reported as the least effective antibiotic in 5 out of 12 studies. This may indicate a consistent pattern of reduced efficacy in treating otitis media in Iraq. Similarly, Ceftriaxone and Penicillin G showed considerable ineffectiveness, each reported as least effective in 4 studies, with ineffectiveness rates of 23.5% and 22.2%, respectively. Although Cefpodoxime showed a 100% ineffectiveness rate, this was based on a single study and thus lacks statistical strength. Azithromycin also demonstrated poor outcomes, being ineffective in 25% of its uses across 12 studies.
A total of 23 studies reported on the antibiotic susceptibility patterns of bacterial pathogens isolated from patients with otitis media. The antibiotics most commonly assessed included Amikacin (n=24), Gentamicin (n=23), Ciprofloxacin (n=22), and Ampicillin (n=20), reflecting a consistent focus on aminoglycosides, fluoroquinolones, and β-lactam agents in empirical and targeted therapy. This frequent utilization likely reflects their broad-spectrum activity and their clinical relevance in managing both Gram-negative and Gram-positive organisms.
Conversely, antibiotics such as Teicoplanin, Cefpodoxime, Minocycline, and Daptomycin were reported in only one or two studies, possibly due to limited accessibility, cost considerations, or their role as second-line or reserve options in resistant infections. The diversity in antibiotic selection across studies suggests heterogeneity in local prescribing practices, diagnostic capacities, and antibiotic stewardship protocols. Furthermore, the moderate representation of Vancomycin, Trimethoprim-Sulfamethoxazole, and Azithromycin indicates their selective application in specific clinical contexts, such as methicillin-resistant Staphylococcus aureus (MRSA) or polymicrobial infections.
Notably, 11 of the included studies did not investigate antibiotic susceptibility. While these studies still contributed valuable epidemiological and clinical insights, their exclusion of antimicrobial profiling limits cross-comparability and highlights the need for comprehensive resistance data in future investigations. Some studies indicated increasing resistance to commonly prescribed antibiotics, such as penicillins, first-generation cephalosporins, and Trimethoprim-Sulfamethoxazole. In contrast, fluoroquinolones (e.g., Ciprofloxacin), aminoglycosides (e.g., Gentamicin), and fourth-generation cephalosporins (e.g., Cefepime) maintained relatively high efficacy against many isolates, particularly Pseudomonas and Staphylococcus species. A few studies also reported resistance to carbapenems among Proteus and Klebsiella isolates, which—if confirmed—would raise concerns about the emergence of multidrug-resistant strains [37]. This highlights the urgent need for antimicrobial stewardship, updated local treatment guidelines, and routine culture and sensitivity testing before initiating empirical therapy.
Research gaps and recommendations
Several critical gaps were noted: lack of standardized protocols across studies, limited use of molecular diagnostic tools to identify resistance genes or virulence factors, absence of comprehensive statistical analyses exploring gender-pathogen associations, and infrequent use of evidence-based antibiograms to guide empirical treatment. To address these gaps, future research should incorporate molecular typing, larger multicenter sample sizes, and unified methodologies. National databases on otitis media pathogens and resistance profiles could also support better clinical decisions and public health strategies.
Limitations
This review was limited by the variability in study designs and reporting standards. Several included studies lacked comprehensive demographic or resistance data, and a standardized quality assessment tool was not applied. Furthermore, molecular data on resistance mechanisms were absent, limiting the depth of resistance characterization. These limitations should be addressed in future research to enhance the comparability and clinical applicability of findings.
Conclusion
Otitis media remains a highly prevalent condition among Iraqi children, particularly males, with cases reported across various governorates. The reviewed data highlight the urgent need for preventive strategies and early screening initiatives, especially in early childhood, where anatomical and immunological vulnerabilities are most pronounced.
Observed variations in microbial profiles and antibiotic susceptibility across cities and time periods suggest evolving bacterial behavior and increasing resistance trends. These findings underscore the necessity of regularly updating national treatment guidelines based on local epidemiological data.
To enhance clinical outcomes and reduce the inappropriate use of antibiotics, it is essential to strengthen the capacity of local laboratories in conducting bacterial cultures and antimicrobial susceptibility testing. Furthermore, the implementation of multicenter studies with larger sample sizes and standardized methodologies is strongly recommended. Such studies should emphasize bacterial isolation, antimicrobial profiling, and molecular characterization of pathogens to support evidence-based clinical management and public health planning.
Recommendations
In light of the findings from this comprehensive review on otitis media in Iraq, the following recommendations are proposed to improve clinical outcomes, curb antimicrobial resistance, and strengthen research infrastructure:
1. Enhance public health education: Launch targeted awareness programs for caregivers and communities to improve recognition of early symptoms of ear infections, promote timely healthcare-seeking behavior, and educate on preventive measures, especially among populations with young children.
2. Implement routine microbiological testing: Prioritize bacterial culture and antimicrobial susceptibility testing before initiating antibiotic therapy, particularly in recurrent or chronic cases. This approach ensures evidence-based treatment, reduces empirical misuse, and limits resistance development.
3. Establish a national antimicrobial resistance surveillance system: Develop and maintain a centralized, nationwide database to monitor bacterial resistance trends across regions. This would serve as a vital tool for guiding treatment protocols and policy decisions.
4. Strengthen laboratory capacity in primary care settings: Equip primary healthcare centers with modern diagnostic tools and trained personnel to facilitate on-site identification of pathogens and guide prompt, appropriate treatment at the community level.
5. Regularly update clinical treatment guidelines: Revise otitis media management protocols periodically to reflect emerging local data on pathogen distribution and resistance profiles, ensuring relevance and effectiveness of therapeutic strategies.
6. Promote integrative, multidisciplinary research: Encourage future studies to include robust statistical and genetic analyses to better define risk factors, microbial virulence mechanisms, and patient-specific predictors of disease severity and recurrence.
7. Regulate antibiotic dispensation and enforce prescribing policies: Enact and enforce legislation to prevent over-the-counter sales of antibiotics without a valid prescription, thereby limiting irrational drug use and mitigating the spread of resistant strains.
8. Support national multicenter research initiatives: Facilitate collaborative, multicenter research projects covering all geographic regions of Iraq to generate comprehensive, representative data that can inform national health policy and tailored interventions.
Declarations
Author’s contributions: The author, Dhafer Rahman Abed Al-Janabi, conducted the investigation, data extraction, data analysis, and writing of the original draft. He also provided the financial support and finalized the manuscript. The author has read and approved the final version of the manuscript.
Funding: No institutional or external funding was received to support this study.
Consent for publication: This article does not contain any identifiable personal data or images.
Competing interests: The author declares no competing interests.
References
- Aldhaher ZA, Hassan HF, Al-Jassim ZG, Mahmood MA. Bacterial isolates and antibiotic susceptibility of ear infections in Iraqi patients. Int J Biosci. 2018; 13: 292–7.
- Al-Hamamy HR, Salih WH, Al-Mudallal NH. Bacterial isolates and antibiotic susceptibility of ear infections in Al-Kindy Teaching Hospital, Baghdad, Iraq. Res J Pharm Technol. 2021; 14: 6503–6.
- Yousif FH, Mohammed SH, Ali MJ. Isolation and identification of bacteria and fungi from patients with otitis media in the city of Hawija and studying the sensitivity of antibiotics to them. J Educ Sci Stud. 2024; 1: 23.
- Ali MK, Wadi FR. Prevalence of asymptomatic Streptococcus pyogenes carriage and antibiotic susceptibility among schoolchildren in Baghdad, Iraq. Int J Des Nat Ecodynamics. 2025; 20: 211–6.
- Mehdi AZ, Al-Hilali HA, Jebur MS. Immunogenetic and bacteriological study of acute otitis media and tonsillitis among children patients. World J Pharm Sci. 2015; 1340–6.
- Alobaidi A, Surhan RK, Alsadawi AA. Identification of methicillin resistant Staphylococcus aureus isolated from chronic suppurative otitis media. J Sci Res Med Biol Sci. 2024; 5: 112–9.
- Kadhim HJ, Al-Dulaimi THK, Kadhim WA, Tolaifeh ZA, Al-Khafaijy NMS. Isolation and identification of some pathogenic bacteria from otitis media in Babylon Governorate. J Glob Pharma Technol. 2018; 12: 433–7.
- Almamory I, Kamal SAA. Bacteria and fungi associated with acute otitis media. J Biol Agric Healthc. 2014; 4: 41–6.
- Abdul APDLA, Lateef D. Effected of xylitol on pneumoniae isolated from province/Iraq. Aust J Basic Appl Sci. 2016; 10: 21–5.
- Azharal-Thahab NJM. Microbial profile from patients with otitis media. Int J Pharm Res. 2019; 11.
- Al-Marzoqi AH, Al-Janabi HSO, Hussein HJ, Al Taee ZM, Yheea SK. Otitis media: etiology and antibiotics susceptibility among children under ten years old in Hillah city, Iraq. J Nat Sci Res. 2013; 3: 2224–3186.
- Alabedi RF, Aljebouri AH, Al-Maaroof ZW. Acute otitis media-associated diarrhea in children less than 2 years old. Open Access Maced J Med Sci. 2022; 10: 1406–10.
- Abdul-Lateef LA, Alturaihy SH, Al-Taai SAAM. Molecular characterization of some virulence factors of Streptococcus pneumoniae isolated from children with acute otitis media in Hilla, Iraq. Br Biotechnol J. 2016; 10: 1–11.
- Al-Hasnawi EA. Isolation of Staphylococcus aureus from ear swab in Iraqi children as a causative agent of otitis externa. J Fac Med Baghdad. 2017; 59: 258–61.
- Al-Rawazq HS, Mohammed AK, Hussein AA. Etiology and antibiotic sensitivity for otitis media in a central pediatric teaching hospital. Iraqi Med J. 2013; 59: 84–90.
- Wadi FR, Ali MK. Isolation and antibiotic sensitivity testing of Pseudomonas aeruginosa isolates from patients with chronic suppurative otitis media in Baghdad. Ibn Al-Haitham J Pure Appl Sci. 2025; 38: 27–36.
- Sarah MS, Ali HF. Staphylococcus aureus isolated from Iraqi pediatrics with.
- Hissab B, Al-Oqaili NAD. Genetic relationship between chronic otitis media infection and TLR4 gene in Al-Qadisyah province, Iraq. Al-Kufa Univ J Biol. 2023; 15: 62–7.
- Mohsen BA, Jwad Alia. Microbiology and drug sensitivity pattern for patients with chronic otitis media in Aldiwanyia Teaching Hospital. Int J Pharm Res. 2020; 12.
- Abdelhameed A, Alharbi N, Algburi A. Genome sequence and assessment of the virulence and antibiotics resistance of a novel Paenibacillus sp. 6A isolated from a patient with acute otites media in Diyala City, Iraq. 2020.
- Algburi A, Abdelhameed A, Naser RH, Alharbi NK, Quinn GA, Popov IV, et al. Antibiotic susceptibility of bacterial isolates from chronic otitis media in Diyala Province, Iraq. AIP Conf Proc. 2024.
- Hassooni HR, Fadhil SF, Hameed RM, Alhusseiny AH, Jadoo SAA. Upper respiratory tract infection and otitis media are clinically and microbiologically associated. J Ideas Health. 2018; 1: 29–33.
- Hasan HA. Antimicrobial sensitivity profile of bacterial agents in chronic suppurative otitis media patients in Samawa City. Int J Health Sci (Qassim). 6: 8178–83.
- Hameed AK, Kareem AS, Khudhur HR. Bacteriological study and antibiotic susceptibility of some bacterial isolates among otitis media patients in Al-Muthanna Province, Iraq. Med J Babylon. 2024; 21: 686–90.
- Almayali E, Al-Kraety IAA, Naji AM, Abd Almunaam LH. Bacteriological study and its antibiotics susceptibility pattern of otitis media in Iraqi patients. Rev Bionatura. 2023; 8: 67.
- Al-Ani R. Prevalence of otitis media among patients attending otorhinolaryngology clinic in Ramadi City, Iraq. Egypt J Ear Nose Throat Allied Sci. 2020; 21: 17–21.
- Al-Ani RM, Al-Zubaidi MI, Lafi SA. Profile of aerobic bacteria and their antibiotic sensitivity in chronic suppurative otitis media in Al-Ramadi Teaching Hospital, Ramadi City, Iraq. Qatar Med J. 2021; 2021: 3.
- Qarani SM. Antibiotic resistance pattern of Streptococcus pneumoniae among infants younger than six months of age with acute otitis media in Erbil city. Diyala J Med. 2022; 22: 81–93.
- Juma ASM, Ubeid MH. A microbiological survey of ear infections in inhabitants of Erbil City. Cihan Univ Sci J. 2022; 6: 62–7.
- Al-Jubouri SNA, Dahham SN. Molecular detection of virulence factors genes for some species of bacteria that cause otitis media in Kirkuk Governorate. J Biosci Appl Res. 2024; 10: 452–65.
- Alshebly BA, Hassan MA. Antibiotics resistances pattern of Escherichia coli and Staphylococcus spp and associated with otitis media and other site of infection. Int Tinnitus J. 2024; 28: 223–7.
- Hateet RR, Banoon SR, Mohammed MM. Isolation and identification of pathogenic bacteria causing otitis media in Misan Governorate. J Pure Appl Microbiol. 2022; 16: 1384–91.
- Kadhum AA. Antibiotic resistance patterns of bacteria isolated from otitis patients. Cent Asian J Med Nat Sci. 2024; 5: 1054–63.
- Arif ED, Muhamed EA, ThairAbdulla X. Isolation and identification of the bacteria causing ear infections and their antimicrobial susceptibility pattern in Sulaymaniyah province.
- Bluestone CD. Eustachian tube: structure, function, role in otitis media. PMPH-USA; 2005.
- Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013; 131: e964–99.
- Tacconelli E. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development. 2017.