
Review ArticleOpen Access, Volume 3 Issue 2
Improving treatment compliance in adult-onset testosterone deficiency by using charts depicting probability of mortality based on algorithms
Mruga M Dhebar1; Richard C Strange2; Geoffrey Hackett3; Sudarshan Ramachandran1,2,4*
1Department of Clinical Biochemistry, University Hospitals Birmingham NHS Foundation Trust, West Midlands, United Kingdom.
2School of Pharmacy and Bioengineering, Keele University, Staffordshire, United Kingdom.
3School of Health and Life Sciences, Aston University, Birmingham, United Kingdom.
4Department of Mechanical and Aerospace Engineering, Brunel University London, United Kingdom.
*Corresponding author: Sudarshan Ramachandran
Department of Clinical Biochemistry, University Hospitals Birmingham NHS Foundation Trust, Good Hope Hospital, Sutton Coldfield, West Midlands B75 7RR, United Kingdom.
Tel: +44-121-424 7246;
Email: sud.ramachandran@uhb.nhs.uk
Received : Jul 28, 2025 Accepted : Sep 03, 2025 Published : Sep 10, 2025
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Ramachandran S © All rights are reserved
Citation: Dhebar MM, Strange RC, Hackett G, Ramachandran S. Improving treatment compliance in adult-onset testosterone deficiency by using charts depicting probability of mortality based on algorithms. Epidemiol Public Health. 2025; 3(2): 1077.
Abstract
Treatment non-adherence is a major problem in the management of chronic pathologies. Research has suggested that education, shared decision making and clear communication were factors that may help mitigate non-adherence. Currently use of many chronic disease therapies is evidence based. Most of the trials carry out complex statistics that are difficult to transmit to the patient. Hence, it is essential to simplify the probability algorithms obtained from regression analyses to aid clarity during the doctor-patient communication. We describe two chronic pathologies (functional hypogonadism and cardiovascular disease prevention) managed in the Metabolic Clinics at the University Hospitals Birmingham NHS Foundation Trust, where graphical illustrations of treatment benefit were created from regression models and used as a communication tool. The BLAST screened cohort audit was coordinated at our secondary care centre and patient level data were available. This allowed us to calculate the probability of mortality for each man with type 2 diabetes and functional hypogonadism using logistic regression analysis. Probability of mortality was plotted against age in men treated/not treated with testosterone replacement and phosphodiesterase 5-inhibitors. Regarding cardiovascular disease prevention, we used the cumulative data from the Cholesterol Treatment Trialist collaboration demonstrating the scale of benefit associated with statins (22% relative risk reduction per 1 mmol/L decrease in low density lipoprotein cholesterol). Other low-density lipoprotein-cholesterol lowering agents have demonstrated similar benefit. An algorithm calculating the relative risk reduction was derived and this was transferred as a graph, enhancing communication clarity. In these two examples we have provided ways in which complex algorithms can be converted graphs that the lay public can easily comprehend.
Keywords: Logistic regression; Gompertz/Makeham equation; Age; Adult-onset hypogonadism; Type 2 diabetes; Testosterone therapy; All-cause mortality; Phosphodiesterase type 5 inhibitors.
Introduction
Treatment adherence of chronic pathologies is essential for optimal health care [1,2]. Non-adherence is considered a major factor contributing to disease severity [3]. It also appears that education and shared decision making by the doctor and patients yield the best results regarding adherence.[3] Cheen et al. studying 539,156 individuals (33 randomised controlled trials, 26 cohort studies and 2 cross sectional studies) with chronic conditions in 2019 found that the non-adherence, defined as not collecting newly initiated therapeutic agents, was 17% [4]. This figure was greater in patients with osteoporosis (25%) and dyslipidaemia (25%) whilst lower in those with diabetes (10%).[4] Foley et al. carried out a systematic review of 178 studies, each study including between 22 and 599,141 individuals suffering two or more chronic pathologies, and studied non-adherence during follow-up [5]. Data was obtained via self-reports, pharmacy data and electronic records. Overall non-adherence was 42.6%, ranging between 7.0% and 83.5% in the individual studies [5]. Kvanstrom et al. determined factors that contributed to medication adherence by analysing data from 89 studies [6]. It was evident that information of the pathology, treatment and communication were predictors of adherence [6]. It appears that education and shared decision making by the doctor and patients yield the best results regarding adherence [3].
Treatment of chronic conditions are increasingly based on evidence-based medicine [7]. Presenting and discussing evidence appears to lead to greater in better understanding of patient management choices, this in turn resulting in improved clinical outcomes [8,9]. Thus, it is essential to develop methods whereby evidence can be translated into practice with evidence informed practice perhaps being a vehicle of evidence transfer to the patient [10]. We now describe two examples of graphical illustrations of risk and treatment benefit (in men with functional hypogonadism/type 2 diabetes (T2DM) and patients referred for cardiovascular disease (CVD) prevention) based on algorithms derived from research data, are presented to the patients attending the Metabolic Clinics at Good Hope Hospital, University Hospitals Birmingham NHS Foundation Trust, West Midlands, United Kingdom.
Functional hypogonadism
Functional hypogonadism (also known as adult-onset testosterone deficiency and testosterone deficiency syndrome) is diagnosed in men demonstrating low serum testosterone levels and symptoms attributed to the low hormone levels, after excluding primary and hypothalamic/pituitary causes and Klinefelter syndrome [11]. The testosterone thresholds used to diagnose functional hypogonadism in the Metabolic Clinics are in accordance with the British Society for Sexual Medicine serum testosterone thresholds; serum Total Testosterone (TT) <12 nmol/L or Free Testosterone (FT) <0.225 nmol/L) checked between 8-11 AM on two separate occasions [11]. Functional hypogonadism has been associated with increased all-cause mortality [12-16]. Importantly testosterone therapy in functional hypogonadism is associated with a reduction in all-cause mortality, especially in men with T2DM [15-17]. Further, Phosphodiesterase 5-Inhibitors (PDE5I) are often prescribed in men with functional dysfunction presenting with erectile dysfunction and the group of drugs have been associated with significant reduction in CVD and all-cause mortality [16,18-20]. Included in the above studies demonstrating reduction in all-cause mortality following TTh and PDE5i use in men with T2DM and functional hypogonadism is the BLAST (Birmingham, Lichfield, Atherstone, Sutton and Tamworth) study, a Randomised Controlled Trial (RCT) with a follow-up of the screened patients (BLAST screened cohort), conducted at University Hospitals Birmingham NHS Foundation Trust, evaluating the effects of testosterone undecanoate on hypogonadal symptoms and metabolic parameters over a 30-week treatment period (RCT phase) and all-cause mortality over a mean 3.8 year follow-up in the total cohort (BLAST screened cohort-audit phase) [16]. The screened cohort included 857 men with T2DM and 537 of these men were diagnosed with functional hypogonadism (two samples demonstrating serum TT ≤12 nmol/l or calculated FT ≤0.25 nmol/l); of these 537 men 175 were commenced on TTh (follow-up: 3.7 years) whilst the remaining 362 men did not have hormone replacement. Of the total cohort, 175 men with erectile dysfunction were prescribed PDE5I. Of the total BLAST screened cohort, 320 men were eugonadal with serum TT >12 nmol/l and calculated FT >0.25 nmol/l [16]. The 320 eugonadal men were at lower risk (mortality: 11.3%) of all-cause mortality (Hazard Ratio (HR): 0.62, 95% Confidence Interval (CI): 0.41-0.94, the Cox regression model adjusted for baseline age) compared to the 362 men with functional hypogonadism not on TTh (mortality: 16.9%) [16]. TTh in the 175 men was significantly associated with lower all-cause mortality (mortality: 3.4%) compared to the 362 untreated men during follow-up (HR: 0.38, CI: 0.16 - 0.90, the Cox regression analysis once again adjusted for age). The 175 men on PDE5I agents appeared at lower risk (mortality: 14.7%) of all all-cause mortality than the men not on these agents (mortality: 1.7%). As the initial date of PDE5I prescribing was unknown, logistic regression was carried out with all-cause mortality as the dichotomous outcome; all-cause mortality in men on PDE5I was significantly lower compared to the men not on the drug (Odds Ratio (OR): 0.06, 95% CI: 0.009–0.47) [16]. This association remained independent (OR: 0.07, 95% CI: 0.009–0.48) of age at final assessment/death, TTh and statin therapy.
Following the above publication, we wished to present the data in a manner, preferably via graphs, that would be easily comprehended by patients to augment understanding of the importance of TTh and PDE5I treatment in men with T2DM and functional hypogonadism. As age is usually a significant predictor of mortality, we decided to determine how TTh and PDE5I altered the association between age and all-cause mortality as described by Gompertz in 1825 [21]. The algorithm developed by Gompertz suggests that mortality rises exponentially with age and is found below [22].
The Gompertz law of mortality underwent a modification by Makeham with the introduction of extrinsic mortality (y) into the algorithm (Gompertz/Makeham model) and is presented below [23].
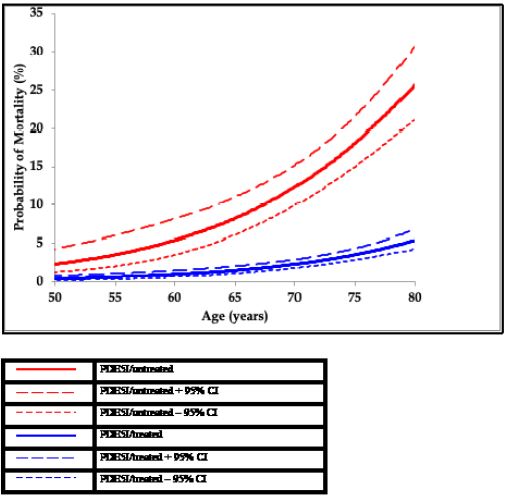
We initially established that in our cohort of 857 men mortality was exponentially related to age; age and Ln of the mortality showed a linear association [21]. Following that logistic (and logit) regression analysis was performed to confirm the association between death/survival (dichotomous dependent variable) and age at death or last clinical assessment as the independent variable (Table 1 – model 1). Subsequently the effect of TTh and PDE5I on the association between age and mortality was evaluated. We used separate logistic regression models (Table 1–Models 2 and 3) with TTh and PDE5I included with age at death or final visit as the independent variables and death as the dependent variable. TTh and PDE5I status as discrete ordinal variables were factorised with one category selected as reference (TTh/untreated and PDE5I/untreated) and the treated groups (TTh/treated and PDE5I/treated) compared. Treatment with TTh (Table 1-Model 2) and PDE5I (Table 1–Model 3) demonstrated significantly lower mortality, compared to their untreated counterparts. To graphically illustrate the impact that treatment had on age related mortality, we calculated the probability of mortality (and 95% CI) for each man using the separate logistic regression models (Table 1–Models 1-3). The probability of mortality for every individual, based on treatment status (treated/untreated) was plotted against age (Figures 2 & 3). This clearly showed that TTh and PDE5I altered the association between age and mortality [21]. Figure 4 demonstrates the Absolute Risk Reduction (ARR) and Relative Risk Reduction (RRR) when a man with functional hypogonadism is on TTh [24].
Patients with functional hypogonadism were referred to the Metabolic Clinics by primary and secondary care physicians and assessed in accordance with the then current BSSM guidelines [11,24,25]. The current evidence based on guidelines was discussed with functional hypogonadism focusing on the benefits and potential adverse effects of treatment [11,25]. In men with T2DM where functional hypogonadism is highly prevalent, the evidence was augmented by Figures 2-4. Figures 2 and 3 very clearly demonstrate the mortality decrease associated with TTh and PDE5I use, whilst Figure 4 adds numerical values (ARR and RRR) to the visual benefit at ages 55 and 65 years. We expected that this graphical display of benefit and the doctor-patient interaction that followed may have improved treatment adherence. It is important that the characteristics of the BLAST screened cohort was emphasised and the patients were aware that the results strictly speaking only applied to men of similar presentation phenotype.
Cardiovascular disease prevention
The results of RCTs investigating CVD reduction associated with drugs such as resins, statins, ezetimibe, Convertase Subtilisin/Kexin Type-9 inhibitors (PCSK9) and bempedoic acid demonstrating associations between LDL-C reduction led to the LDL-C hypothesis [27,28]. Patients at high risk of CVD are referred to the Metabolic Clinic at Good Hope Hospital for lipid lowering therapy, with the principal aim to lower density Lipoprotein-cholesterol (LDL-C) below targets published [29]. Our discussion with the patients centered on the Cholesterol Treatment Trialist (CTT) collaboration which analysed CVD prevention in 26 statin trials; 5 trials (39,612 patients) compared statins with greater vs lesser efficacy (type or dose) and the remaining 21 trials (129,526 patients) compared statins vs placebo [30]. Both statin vs statin and statin vs placebo trials yielded similar CVD outcomes and the analysis showed a CVD RRR of 22% (rate ratio = 0.78) per 1.0 mmol/L decrease in LDL-C (rate ratio: 0·78, 95% CI: 0.76–0.80; p<0·0001) [30]. Importantly, non-statin RCTs using ezetimibe (SHARP, IMPROVE-IT) [31,32], Proprotein Convertase Subtilisin/Kexin Type-9 inhibitors (FOURIER, ODESSEY) [33,34], and bempedoic acid [28], all these agents lowering LDL-C via varying mechanisms decreased CVD risk, comparable to the results of the CTT Collaboration after adjusting the analysis for follow-up.
We used the results from the CTT collaboration and derived the following equation to calculate RRR for each individual patient, this dependent on the LDL-C reduction following treatment [35].

Figure 5, which is based on equation 3, clearly shows the patient the CVD RRR that could be expected from LDL-C lowering. We could not create an age vs probability of CVD graph, similar to that carried out in functional hypogonadism using the BLAST screened cohort data (Figures 2-4), as individual patient level data were not available. However, once again the graphical illustration of evidence provides a clear message and promotes doctor-patient dialogue and discussion which may improve treatment adherence.
In this review we highlight 2 examples where easy to understand graphs were created from algorithms derived from clinical trials. Most clinical outcomes can be displayed using the techniques that we have (Figures 2-4 with patient level data and Figure 5 with grouped data). Both functional hypogonadism and CVD are highly prevalent, hence even modest improvements in adherence can yield major benefits.
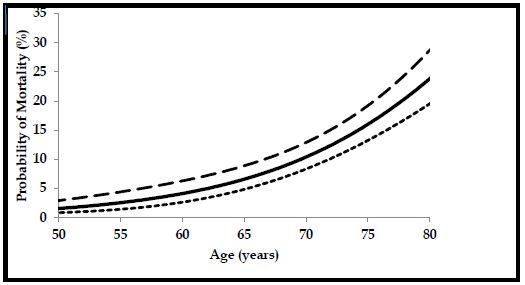
This figure is taken from Hackett G, Jones PW, Strange RC, Ramachandran S. Statin, testosterone and phosphodiesterase 5-inhibitor treatments and age-related mortality in diabetes. World J Diabetes. 2017 Mar 15; 8(3): 104-111. (Reproduced with permission from Baishideng Publishing Group under the terms of Creative Commons Attribution License)
This figure is adapted from Hackett G, Jones PW, Strange RC, Ramachandran S. Statin, testosterone and phosphodiesterase 5-inhibitor treatments and age-related mortality in diabetes. World J Diabetes. 2017 Mar 15; 8(3): 104-111. (Reproduced with permission from Baishideng Publishing Group under the terms of Creative Commons Attribution License)
This figure is adapted from Hackett G, Jones PW, Strange RC, Ramachandran S. Statin, testosterone and phosphodiesterase 5-inhibitor treatments and age-related mortality in diabetes. World J Diabetes. 2017 Mar 15;8(3):104-111. (Reproduced with permission from Baishideng Publishing Group under the terms of Creative Commons Attribution License).
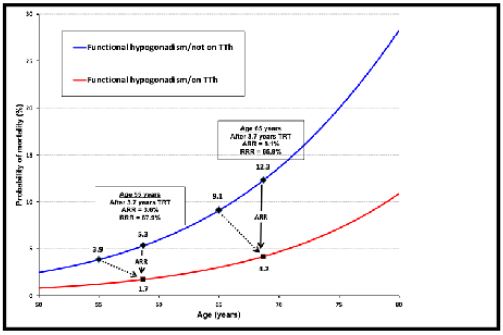
This figure is adapted from Ramachandran S, Hackett GI, Strange RC. Hypogonadism in men with diabetes: Should testosterone replacement therapy be based on evidence-based testosterone levels and lifetime risk reduction? Edorium J Biochem 2017; 2: 1-3. (Reproduced with permission from Edorium Journals under the terms of Creative Commons Attribution License)
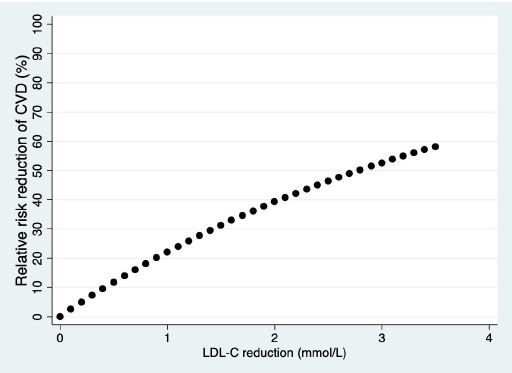
This figure is adapted from König CS, Mann A, McFarlane R, Marriott J, Price M, Ramachandran S. Age and the Residual Risk of Cardiovascular Disease following Low Density Lipoprotein-Cholesterol Exposure. Biomedicines. 2023 Dec 2;11(12):3208. (Reproduced with permission from Biomedicines, MDPI under the terms of Creative Commons Attribution License)
Author declarations
Author contributions: SR, RCS, GH and MMD planning of the paper, preparation of manuscript.
Disclosures: None regarding this paper.
References
- Mir TH. Adherence Versus Compliance. HCA Healthc J Med. 2023;4(2):219-220. doi: 10.36518/2689-0216.1513.
- Aremu TO, Oluwole OE, Adeyinka KO, Schommer JC. Medication Adherence and Compliance: Recipe for Improving Patient Outcomes. Pharmacy (Basel). 2022;10(5):106. doi: 10.3390/pharmacy10050106.
- Driever EM, Brand PLP. Education makes people take their medication: myth or maxim? Breathe (Sheff). 2020;16(1):190338. doi: 10.1183/20734735.0338-2019.
- Cheen MHH, Tan YZ, Oh LF, Wee HL, Thumboo J. Prevalence of and factors associated with primary medication non-adherence in chronic disease: A systematic review and meta-analysis. Int J Clin Pract. 2019;73(6):e13350. doi: 10.1111/ijcp.13350.
- Foley L, Larkin J, Lombard-Vance R, Murphy AW, Hynes L, Galvin E, Molloy GJ. Prevalence and predictors of medication non-adherence among people living with multimorbidity: a systematic review and meta-analysis. BMJ Open. 2021;11(9):e044987. doi: 10.1136/bmjopen-2020-044987.
- Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research. Pharmaceutics. 2021;13(7):1100. doi: 10.3390/pharmaceutics13071100.
- Tenny S, Varacallo MA. Evidence-Based Medicine. StatPearls [Internet]. 2025 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470182/
- O’Connor AM, Wennberg JE, Legare F, Llewellyn-Thomas HA, Moulton BW, Sepucha KR, Sodano AG, King JS. Toward the ‘tipping point’: decision aids and informed patient choice. Health Aff (Millwood). 2007;26(3):716-25. doi: 10.1377/hlthaff.26.3.716.
- O’Connor AM, Llewellyn-Thomas HA, Flood AB. Modifying unwarranted variations in health care: shared decision making using patient decision aids. Health Aff (Millwood). 2004;Suppl Variation:VAR63-72. doi: 10.1377/hlthaff.var.63.
- Kumah EA, McSherry R, Bettany-Saltikov J, van Schaik P. Evidence-informed practice: simplifying and applying the concept for nursing students and academics. Br J Nurs. 2022;31(6):322-330. doi: 10.12968/bjon.2022.31.6.322.
- Hackett G, Kirby M, Rees RW, Jones TH, Muneer A, Livingston M, et al. The British Society for Sexual Medicine Guidelines on Male Adult Testosterone Deficiency. World J Mens Health. 2023;41(3):508-537. doi: 10.5534/wjmh.221027.
- Pye SR, Huhtaniemi IT, Finn JD, Lee DM, O’Neill TW, Tajar A, et al. Late-onset hypogonadism and mortality in aging men. J Clin Endocrinol Metab. 2014;99(4):1357-66. doi: 10.1210/jc.2013-2052.
- Antonio L, Wu FCW, Moors H, Matheï C, Huhtaniemi IT, Rastrelli G, et al. Erectile dysfunction predicts mortality in middle-aged and older men independent of sex steroid status. Age Ageing. 2022;51(4):afac094. doi: 10.1093/ageing/afac094.
- Holmboe SA, Skakkebæk NE, Juul A, Scheike T, Jensen TK, Linneberg A, et al. Individual testosterone decline and future mortality risk in men. Eur J Endocrinol. 2018;178(1):123-130. doi: 10.1530/EJE-17-0280.
- Muraleedharan V, Marsh H, Kapoor D, Channer KS, Jones TH. Testosterone deficiency increases mortality risk and TRT improves survival in type 2 diabetes. Eur J Endocrinol. 2013;169(6):725-33. doi: 10.1530/EJE-13-0321.
- Hackett G, Heald AH, Sinclair A, Jones PW, Strange RC, Ramachandran S. Serum testosterone, TRT and all-cause mortality in type 2 diabetes. Int J Clin Pract. 2016;70(3):244-53. doi: 10.1111/ijcp.12779.
- Shores MM, Smith NL, Forsberg CW, Anawalt BD, Matsumoto AM. Testosterone treatment and mortality. J Clin Endocrinol Metab. 2012;97(6):2050-8. doi: 10.1210/jc.2011-2591.
- Mann A, Strange RC, König CS, Hackett G, Haider A, Haider KS, et al. Testosterone replacement therapy and mortality in high-risk men. Andrology. 2024;12(6):1389-1397. doi: 10.1111/andr.13582.
- Anderson SG, Hutchings DC, Woodward M, Rahimi K, Rutter MK, et al. PDE5 inhibitor use in type 2 diabetes reduces all-cause mortality. Heart. 2016;102:1750-1756. doi: 10.1136/heartjnl-2015-309223.
- Kloner RA, Stanek E, Desai K, Crowe CL, Paige Ball K, Haynes A, Rosen RC. Tadalafil and reduced MACE/mortality. Clin Cardiol. 2024;47(2):e24234. doi: 10.1002/clc.24234.
- Hackett G, Jones PW, Strange RC, Ramachandran S. Statin, testosterone and PDE5-inhibitor treatments in diabetes mortality. World J Diabetes. 2017;8(3):104-111. doi: 10.4239/wjd.v8.i3.104.
- Kirkwood TB. Commentary on Gompertz law. Philos Trans R Soc Lond B Biol Sci. 2015;370:20140379. doi: 10.1098/rstb.2014.0379.
- Hallén A. Makeham’s addition to Gompertz law re-evaluated. Biogerontology. 2009;10(4):517-22. doi: 10.1007/s10522-008-9184-0.
- Hackett G, Kirby M, Edwards D, Jones TH, Rees J, Muneer A. UK policy statements on testosterone deficiency. Int J Clin Pract. 2017;71:e12901. doi: 10.1111/ijcp.12901.
- Hackett G, Kirby M, Wylie K, Heald A, Ossei-Gerning N, Edwards D, Muneer A. BSSM ED guidelines (2017). J Sex Med. 2018;15:430-457. doi: 10.1016/j.jsxm.2018.01.023.
- Kapoor D, Aldred H, Clark S, Channer KS, Jones TH. Hypogonadism assessment in type 2 diabetes. Diabetes Care. 2007;30:911-7. doi: 10.2337/dc06-1426.
- Ramachandran S, Bhartia M, König CS. The lipid hypothesis: PCSK9 inhibitors. Front Cardiovasc Drug Discov. 2020;5:48-81.
- Nissen SE, Lincoff AM, Brennan D, Ray KK, Mason D, et al. Bempedoic Acid in statin-intolerant patients. N Engl J Med. 2023;388:1353-1364. doi: 10.1056/NEJMoa2215024.
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, et al. 2019 ESC/EAS dyslipidaemia guidelines. Eur Heart J. 2020;41:111-188. doi: 10.1093/eurheartj/ehz455.
- CTT Collaboration; Baigent C, Blackwell L, Emberson J, et al. Intensive LDL-lowering meta-analysis. Lancet. 2010;376:1670-81. doi: 10.1016/S0140-6736(10)61350-5.
- SHARP Investigators; Baigent C, Landray MJ, Reith C, et al. Simvastatin + ezetimibe in CKD. Lancet. 2011;377:2181-92. doi: 10.1016/S0140-6736(11)60739-3.
- Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, Darius H, Lewis BS, Ophuis TO, Jukema JW, De Ferrari GM, Ruzyllo W, De Lucca P, Im K, Bohula EA, Reist C, Wiviott SD, Tershakovec AM, Musliner TA, Braunwald E, Califf RM; IMPROVE-IT Investigators. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015;372(25):2387-97. doi:10.1056/NEJMoa1410489.
- Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, Kuder JF, Wang H, Liu T, Wasserman SM, Sever PS, Pedersen TR; FOURIER Steering Committee and Investigators. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017;376(18):1713-1722. doi:10.1056/NEJMoa1615664.
- Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, Edelberg JM, Goodman SG, Hanotin C, Harrington RA, Jukema JW, Lecorps G, Mahaffey KW, Moryusef A, Pordy R, Quintero K, Roe MT, Sasiela WJ, Tamby JF, Tricoci P, White HD, Zeiher AM; ODYSSEY OUTCOMES Committees and Investigators. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N Engl J Med. 2018;379(22):2097-2107. doi:10.1056/NEJMoa1801174.
- König CS, Mann A, McFarlane R, Marriott J, Price M, Ramachandran S. Age and the Residual Risk of Cardiovascular Disease following Low Density Lipoprotein-Cholesterol Exposure. Biomedicines. 2023;11(12):3208. doi:10.3390/biomedicines11123208.